Pulmonary embolism: causes, symptoms, diagnosis and treatment
Pulmonary embolism is an obstruction of blood flow to the lungs, most often from a traveling blood clot; this article explains causes, symptoms, diagnosis, management, and prevention.
A pulmonary embolism (PE) occurs when material—most commonly a blood clot—travels through the circulation and lodges in an artery of the lungs, obstructing blood flow. The consequence is impaired oxygen exchange and increased strain on the right side of the heart. Severity ranges from small, clinically silent emboli to large, life-threatening blockages that reduce oxygen delivery to tissues.
Image gallery
10 Images







Causes and mechanism
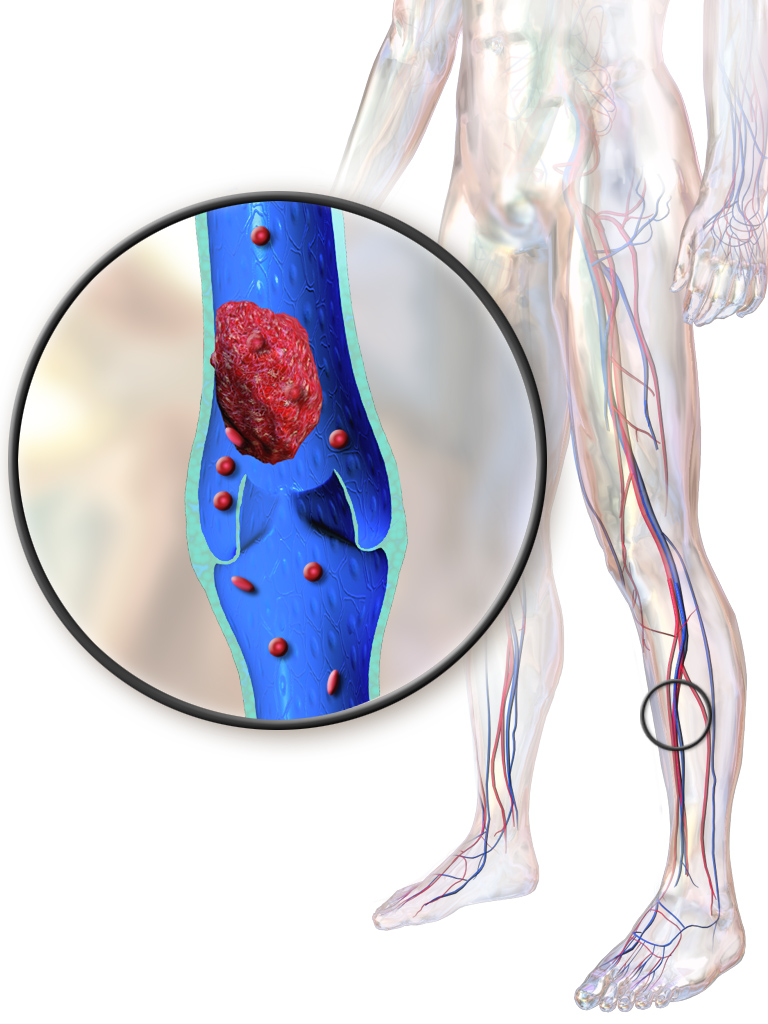
Most pulmonary emboli originate from clots in the deep veins of the legs or pelvis; pieces break free and are carried to the pulmonary arterial circulation. Other types of embolic material include clumped cancer cells, fragments of tumor or invasive growths (tumor emboli), fat released after fractures of large bones, and rarely bone marrow or amniotic fluid in specific settings. The lodgment site, embolus size, and the patient’s existing cardiopulmonary reserve determine clinical impact.
Risk factors and pathophysiology
Factors that increase the risk of clot formation include prolonged immobility, recent surgery or trauma, active cancer, pregnancy and the postpartum period, use of certain hormonal therapies, and inherited or acquired clotting disorders. When an embolus obstructs a pulmonary artery, it raises pulmonary vascular resistance, can reduce left ventricular preload, and may precipitate low blood pressure and shock in severe cases.
Symptoms and clinical features
Symptoms often appear suddenly and can include shortness of breath, chest pain that may worsen with breathing, rapid breathing or heart rate, coughing (sometimes with blood-streaked sputum), lightheadedness, or fainting. Small emboli may cause minimal or nonspecific symptoms and be detected incidentally.
Diagnosis
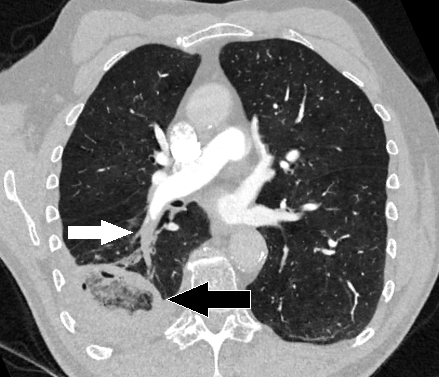
Diagnosis typically combines a clinical assessment with imaging and laboratory tests. Common tools include pulse oximetry, blood tests such as D-dimer when suspicion is low to moderate, chest imaging like computed tomography pulmonary angiography, ventilation–perfusion scanning, and ultrasound of the legs to seek a source clot. Clinical scoring systems help guide testing and urgency of treatment.
Treatment and prevention
- Initial treatment often focuses on anticoagulation to stop further clot growth and allow natural clot breakdown.
- In large or life-threatening emboli, thrombolytic drugs, catheter-directed clot removal, or surgical embolectomy may be considered.
- Supportive care includes oxygen and hemodynamic support when needed.
- Prevention targets risk factors: early mobilization after surgery, use of compression devices, appropriate anticoagulant prophylaxis in high-risk patients, and managing underlying conditions such as malignancy.
Complications and outlook
Complications include persistent shortness of breath, chronic thromboembolic pulmonary hypertension in a minority of cases, and right heart dysfunction. Prompt recognition and treatment improve outcomes, and long-term management may require extended anticoagulation depending on underlying risk. For reliable patient information and clinical resources, see related guidance and summaries at lung health, professional guidelines at vascular care, and specialist oncology or trauma sources for non-thrombotic emboli referenced here and here. Additional practical advice on fracture-related emboli and fat embolism can be found here and here.
Origin
In up to 80% of all cases, a blood clot causing a pulmonary embolism develops in the deep veins of the leg or pelvis and travels via the inferior vena cava, the right atrium and ventricle of the heart into both pulmonary arteries. As it progresses, the thrombus becomes lodged and occludes the vessel. The larger the thrombus, the larger the area of the lung behind it that is no longer supplied with blood. Often there are several thrombi which block pulmonary vessels completely or partially at the same time or at intervals.
Both lungs of a patient can also be affected. Amniotic fluid embolisms can also occur
during birth, and fat embolisms in the case of fractures of the long tubular bones (e.g. femur). Even bone marrow embolisms are possible in the lungs. Furthermore, air or other gases (e.g. CO2 during laparoscopy) can enter the venous vascular system during injuries or medical procedures.
Pulmonary embolism is one of the most commonly overlooked causes of death.
The lethality of an untreated severe pulmonary embolism is very high at 30 %. Immediate treatment can reduce mortality to 2-8%.

Pathophysiology
The embolus blocks one or more branches of the pulmonary arteries. The larger the internal diameter of the affected vessel, the more serious this becomes. The congestion of blood in front of the thrombus leads to a more or less severe increase in pressure in the pulmonary circulation (pulmonary hypertension) and thus to a strain on the right part of the heart, which may cause it to fail partially or even completely. If the right side of the heart does not fail, there is nevertheless at least a reduction in the amount of blood that can pass through the lungs and reach the left side of the heart. However, the left side of the heart can only pump as much blood as it receives. The consequence of the reduced blood flow is a reduced oxygen supply to the important organs. This can lead to (cardiogenic) shock. Depending on the extent, there may be a lower oxygen content in the blood - hypoxaemia.
A sudden severe pulmonary embolism is called fulminant. The leading symptom is failure of the right heart (right heart failure), accompanied by severe hypoxaemia.
Smaller pulmonary embolisms can also lead to right heart problems. Here, the increase in pressure in the small circulation is not as severe, and the acute survival rate of patients is therefore also significantly higher. In most cases, the thrombi are broken down and the vascular system is thus cleared again. Nevertheless, some patients (especially those with recurrent small pulmonary embolisms) may develop chronic pulmonary hypertension in the further course. This can then be a case of CTEPH.
Following the acute event, an infection of the lung tissue that is no longer sufficiently supplied with blood can lead to a so-called infarct pneumonia. The lung area behind the embolus can infarct, especially after a major embolism with destruction of part of the connective tissue underlying the lung. Despite the high regenerative capacity of the lung tissue, entire areas then die permanently. If the organism survives this, functionless scars develop. If larger areas are affected with a corresponding loss of function, the result is shortness of breath, reduced resilience and often a permanent cough. The facilitated invasion of germs into the initially necrotic, subsequently fibrotically altered - and for antibiotics largely inaccessible - scar tissue also leads later more frequently to pneumonia. The fibrotic remodeling processes also slightly increase the risk of later lung cancer. There is a high rate of late complications, especially with renewed embolisms.
Questions and answers
Q: What is a pulmonary embolism?
A: A pulmonary embolism is a clot of material that blocks blood from getting to the lungs.
Q: What usually causes a pulmonary embolism?
A: It is usually caused by a blood clot that starts somewhere else in the body and travels to the lungs.
Q: Can a pulmonary embolism be caused by something other than a blood clot?
A: Yes, it can also be caused by clumped cancer cells, fat, or bone.
Q: How rare is it for a woman to get a clot of amniotic fluid while giving birth?
A: It is a rare occurrence for a woman to get a clot of amniotic fluid while giving birth.
Q: What are the symptoms of a pulmonary embolism?
A: Symptoms of a pulmonary embolism include sudden shortness of breath, chest pain, and coughing up blood.
Q: How is a pulmonary embolism treated?
A: Treatment for a pulmonary embolism may include medications to thin the blood, oxygen therapy, and in severe cases, surgery.
Q: Can a pulmonary embolism be prevented?
A: Steps that can be taken to prevent a pulmonary embolism include regular exercise, avoiding prolonged sitting, maintaining a healthy weight, and wearing compression stockings if recommended by a doctor.
Related articles
Author
AlegsaOnline.com Pulmonary embolism: causes, symptoms, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/80020
Sources
- nhlbi.nih.gov : "How is Pulmonary Embolism Treated?"
- nhlbi.nih.gov : "What are the Signs and Symptoms of Pulmonary Embolism?"
- doi.org : 10.1111/j.1538-7836.2011.04189.x
- mayoclinic.org : "Pulmonary Embolism – Risk Factors"