Prenatal diagnosis refers to medical tests performed during pregnancy to assess the health and development of the embryo or fetus. These procedures are offered to pregnant women and others carrying a pregnancy to identify structural anomalies, chromosomal changes and certain inherited conditions affecting the child. The information produced by prenatal testing may guide medical management, birth planning, decisions about pregnancy continuation, or preparation for a baby with special needs.
Methods: non-invasive and invasive
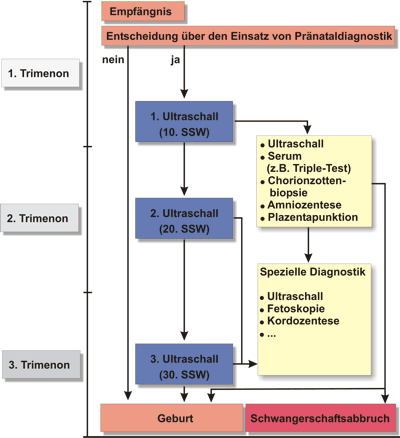
Broadly, prenatal testing falls into two categories. Non-invasive options evaluate maternal blood or use imaging and pose no direct risk to the pregnancy. Common non-invasive approaches include sonographic examination with ultrasound and laboratory screening of maternal serum; newer techniques analyse cell-free fetal DNA in maternal blood. Invasive diagnostic procedures obtain fetal or placental material and carry a small risk of miscarriage. Examples are amniocentesis and chorionic villus sampling, which sample amniotic or placental tissue and fluid (placental sampling or amniotic fluid testing). Timing varies: screening tests are often done in the first or second trimester, while definitive diagnostic tests are typically performed later.
What conditions are tested
Tests target a range of problems, from chromosomal abnormalities to single-gene disorders and structural defects. Screening and diagnostic programs commonly address:
- Down syndrome and other aneuploidies
- Neural tube defects such as spina bifida
- Cleft lip and palate and other structural malformations
- Tay–Sachs disease, cystic fibrosis, and other inherited metabolic or respiratory conditions
- Sickle-cell disease and thalassaemia
- Fragile X syndrome and other single-gene disorders
Clinical uses and outcomes
Results from prenatal diagnosis can be used to refine prenatal care, arrange specialist delivery facilities, initiate in utero or early postnatal treatment when available, or help families prepare emotionally and practically for a child with special needs. In some settings, findings influence the consideration of pregnancy termination (abortion), though legal and cultural responses vary. Screening may also detect non-pathological traits; for example, identification of fetal sex can lead to sex-selective practices in certain regions when a fetus is identified as female.
Risks, counseling, and decision-making
Invasive tests carry procedural risks and all testing has psychological and ethical implications. Pre-test counseling is recommended so people understand the scope and limits of results, possible false positives or negatives, and follow-up options. Genetic counseling helps interpret findings in the context of family history and reproductive choices. Where available, multidisciplinary teams assist with prognosis, treatment options and coordination of care after birth.
Ethical, legal and social considerations
Advances in prenatal technology have raised complex questions, including concerns about reproductive autonomy, privacy, disability rights, and social pressure toward particular reproductive outcomes. Debates over so-called designer babies reflect worries about selecting non-medical traits and widening inequalities. Policymakers, clinicians and ethicists also examine the ethical issues of access, consent and the potential for discrimination. The balance between offering useful clinical information and protecting individual and societal values continues to shape practice and regulation worldwide.
For people considering prenatal testing, authoritative counseling and accurate, balanced information are essential. Further reading and local guidance are available through clinical services and professional organizations (see resources for pregnant people, fetal medicine, birth defect registries, genetic disorder references, ultrasound guidance, diagnostic sampling, Down syndrome information, Tay–Sachs resources, sickle-cell resources, thalassaemia support, cystic fibrosis guidance, Fragile X information, termination law, sex selection discussions, emerging reproductive technologies, ethical analyses).