Pituitary gland: structure, function, development, and clinical relevance
A concise encyclopedia entry on the pituitary gland (hypophysis): its anatomy, lobes and hormones, control by the hypothalamus, development, and key clinical conditions and treatments.
Overview
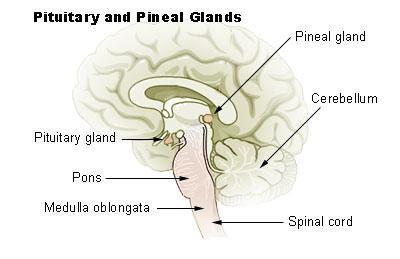
The pituitary gland, also called the hypophysis, is a small but crucial endocrine organ located at the base of the brain, in a bony cavity beneath the optic chiasm. It is often described as a master gland because many of its secretions regulate other endocrine organs. Anatomically and functionally it is tightly linked to the endocrine system and to the hypothalamus, the brain region that controls its activity.
Image gallery
7 Images




Structure and major parts
The gland has two principal portions with distinct origins and roles: the anterior pituitary (adenohypophysis) and the posterior pituitary (neurohypophysis). These are connected to the brain by the pituitary stalk or infundibulum. The anterior lobe is glandular tissue that receives hormonal-releasing and -inhibiting signals delivered from the hypothalamus through a specialized portal blood system. The posterior lobe is neural tissue that stores and releases hormones produced in hypothalamic neurons.
Principal hormones and targets
Each lobe releases several important hormones that affect growth, metabolism, reproduction and fluid balance. Major anterior pituitary hormones include:
- Growth hormone (GH) — acts on bones, muscle and metabolism.
- Adrenocorticotropic hormone (ACTH) — stimulates the adrenal cortex.
- Thyroid-stimulating hormone (TSH) — controls thyroid gland activity.
- Gonadotropins (LH and FSH) — regulate ovarian and testicular function.
- Prolactin — primarily affects lactation and reproductive tissues.
The posterior pituitary releases hormones synthesized in the hypothalamus: antidiuretic hormone (ADH, vasopressin), which influences kidney water reabsorption and blood pressure, and oxytocin, involved in childbirth and certain social behaviors.
Control, development, and relationships
The hypothalamus exerts tight control through neural connections and blood-borne releasing or inhibiting factors. Neurosecretory cells in the hypothalamus send axons and chemical signals down the infundibulum; these neurosecretory cells are essential for coordinated pituitary output. Embryologically, the anterior lobe arises from oral ectoderm (Rathke's pouch) while the posterior lobe develops from neural ectoderm, reflecting their different functions. The gland sits at the base of the brain and is frequently described in relation to adjacent structures such as the optic apparatus and cavernous sinuses.
Clinical importance and examples
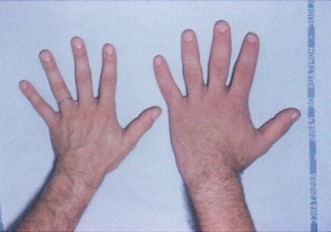
Dysfunction of the pituitary can produce a wide range of conditions. Insufficient hormone production (hypopituitarism) leads to deficits in growth, reproduction, thyroid and adrenal function. Excess secretion from pituitary cells can cause disorders such as acromegaly (excess GH) or Cushing-like syndromes (excess ACTH). Compression by benign tumors (pituitary adenomas) may also impair vision or cranial nerve function. Problems with posterior pituitary hormones can produce diabetes insipidus or inappropriate antidiuretic hormone secretion.
Diagnosis, treatment and notable facts
Evaluation combines clinical assessment, hormone assays and imaging. Many pituitary lesions are approached surgically through a transsphenoidal corridor to the sella turcica. Medical therapies include hormone replacement, dopamine agonists for prolactinomas, and other targeted agents. Although labeled the 'master gland', the pituitary itself is regulated by the hypothalamus and subject to feedback from peripheral endocrine organs, a dynamic network emphasized in modern endocrinology texts referenced at further resources and clinical reviews (hormone summaries, system overviews). For foundational anatomy and cellular control, see materials on the anatomical base and the role of neurosecretory cells.
Questions and answers
Q: What is the pituitary gland?
A: The pituitary gland is a vital part of the endocrine system that is located at the base of the brain between the eyes.
Q: What is the function of the pituitary gland?
A: The pituitary gland controls many important functions in the body by secreting hormones.
Q: How is the pituitary gland attached to the brain?
A: The pituitary gland is attached to the hypothalamus, which is also a gland.
Q: What are the two parts of the pituitary gland?
A: The pituitary gland consists of the anterior pituitary and the posterior pituitary.
Q: What is the pituitary stalk?
A: The pituitary stalk, also called the infundibulum, is the link between the hypothalamus and the pituitary gland.
Q: What controls the endocrine cells of the anterior pituitary?
A: The endocrine cells of the anterior pituitary are controlled by regulatory hormones released by neurosecretory cells in the hypothalamus.
Q: Is the pituitary gland completely independent in its functioning?
A: No, even though it is known as the 'master' endocrine gland, both of the lobes of the pituitary gland are under the control of the hypothalamus.
Related articles
Author
AlegsaOnline.com Pituitary gland: structure, function, development, and clinical relevance Leandro Alegsa
URL: https://en.alegsaonline.com/art/77165
Sources
- genscript.com : genscript.com/product_003/molecular_biology_glossary/id/10470/category/glossary/median_em…
- ncbi.nlm.nih.gov : "Signaling mechanisms in pituitary morphogenesis and cell fate determination"
- pubmed.ncbi.nlm.nih.gov : 10600709