Peptic ulcer: causes, symptoms, diagnosis and treatment
A peptic ulcer is a sore in the stomach or first part of the small intestine. This article explains causes, symptoms, diagnosis, treatment, and differences between gastric and duodenal ulcers.
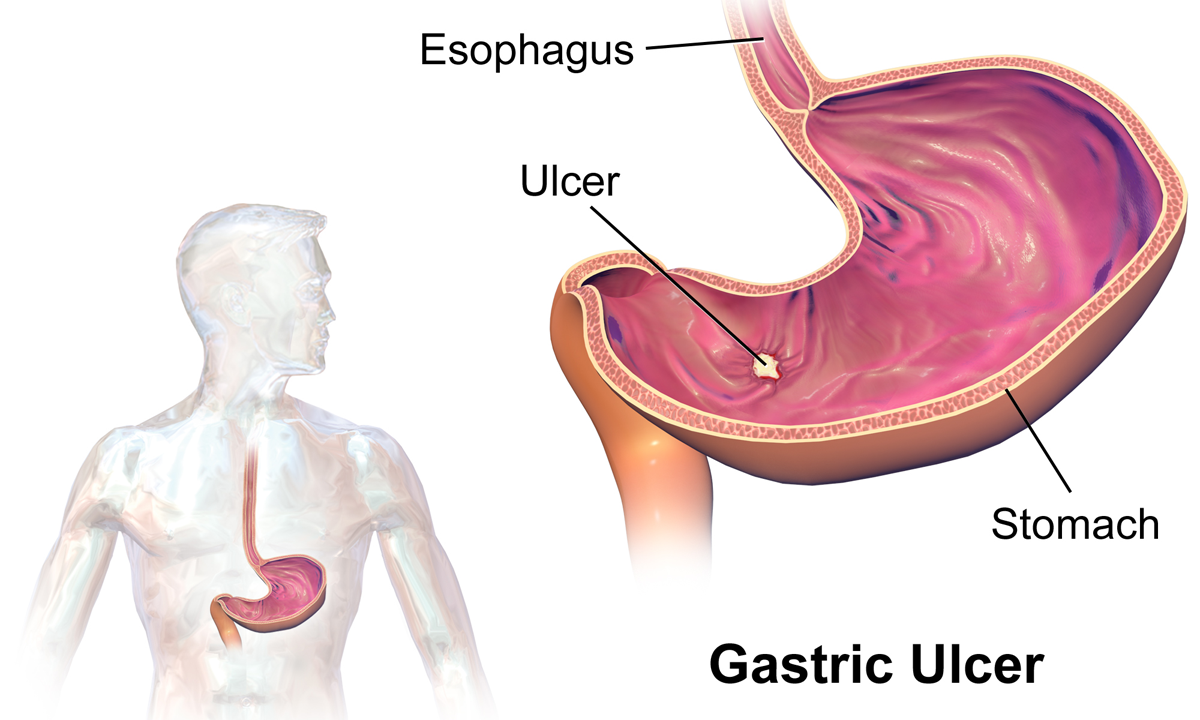
A peptic ulcer is a break in the lining of the stomach or the duodenum, the first segment of the small intestine. Ulcers form where digestive acids and enzymes damage the protective mucous layer, allowing sores to develop in the wall of the gastrointestinal tract. They are common worldwide and range from small, easily treated lesions to large ulcers that can cause serious complications.
Image gallery
10 Images






Characteristics and common causes
Peptic ulcers occur in two main sites: the stomach (gastric ulcers) and the duodenum (duodenal ulcers). Their development is usually linked to an imbalance between aggressive factors—such as stomach acid and pepsin—and defensive mechanisms like mucus and blood flow to the mucosa. Typical causes and risk factors include:
- Helicobacter pylori infection, a bacterium that weakens the mucosal defenses.
- Long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs), which reduce protective prostaglandins.
- Smoking, excess alcohol, and severe physiological stress can increase risk.
- Less commonly, certain medical conditions or medications that increase acid production.
Signs, complications, and diagnosis
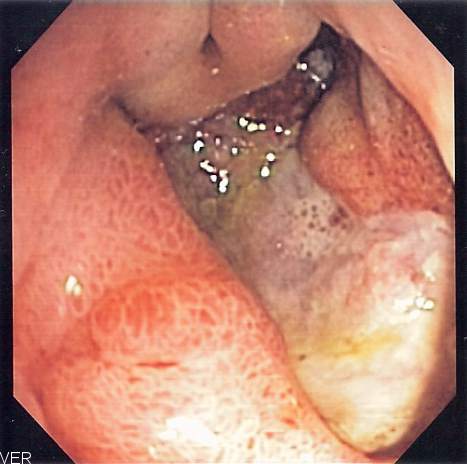
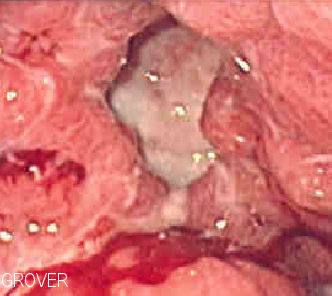
Common symptoms include burning or gnawing epigastric pain, often related to meals, bloating, nausea, or early satiety. More concerning signs are vomiting blood, dark (tarry) stools from bleeding, sudden severe abdominal pain from perforation, or symptoms of obstruction. Diagnosis typically uses endoscopic inspection and biopsy when needed, and noninvasive tests for H. pylori such as breath or stool antigen tests. Imaging and laboratory tests can evaluate complications.
Treatment and prevention
Treatment aims to relieve symptoms, heal the ulcer, eradicate H. pylori when present, and prevent recurrence. Standard approaches include acid suppression with proton pump inhibitors, combined antibiotic regimens to eradicate H. pylori, and stopping or modifying NSAID use. Lifestyle changes—smoking cessation, limiting alcohol, and conservative use of irritating medications—help prevent recurrence. Surgery is now uncommon but may be necessary for uncontrolled bleeding, perforation, or obstruction.
History, distinctions and notable facts
Understanding of peptic ulcer disease changed in the late 20th century when researchers established the role of H. pylori in many cases, shifting treatment from long-term antacid strategies toward curative antibiotic-based regimens. Clinically, gastric ulcers are more likely to be associated with weight loss and may be evaluated carefully to exclude malignancy, whereas duodenal ulcers often cause pain that improves with food. Both types require appropriate diagnosis and follow-up.
For basic definitions, see links for stomach and duodenum. Accurate diagnosis and early treatment reduce the risk of serious outcomes and improve quality of life for affected people.
Questions and answers
Q: What is a peptic ulcer?
A: A peptic ulcer is an ulcer found in the stomach or duodenum.
Q: Where is the duodenum located?
A: The duodenum is the first part of the small intestines and located right after the stomach.
Q: What does the word "peptic" mean?
A: The word "peptic" means related to the stomach.
Q: What is a gastric ulcer?
A: A gastric ulcer is a type of peptic ulcer found in the stomach.
Q: What is a duodenal ulcer?
A: A duodenal ulcer is a type of peptic ulcer found in the duodenum.
Q: How is food processed in the duodenum?
A: The duodenum is the tube that food goes through after it leaves the stomach to be further digested and absorbed in the small intestine.
Q: What is the difference between a gastric and a duodenal ulcer?
A: A gastric ulcer is found in the stomach, while a duodenal ulcer is found in the duodenum.
Related articles
Author
AlegsaOnline.com Peptic ulcer: causes, symptoms, diagnosis and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/75718