Myocardial infarction (heart attack): causes, symptoms, and care
Myocardial infarction, commonly called a heart attack, is death of heart muscle due to interrupted blood flow. This article covers causes, signs, diagnosis, treatment, complications and prevention.
Myocardial infarction, often shortened to MI and commonly known as a heart attack, occurs when blood supply to part of the heart is suddenly interrupted and cardiac muscle tissue is damaged or dies. The interruption typically results from blockage in a coronary artery and produces a spectrum of symptoms and consequences, from transient chest discomfort to life‑threatening collapse. Rapid recognition and treatment reduce the amount of muscle lost and improve survival.
Image gallery
10 Images







What happens and why
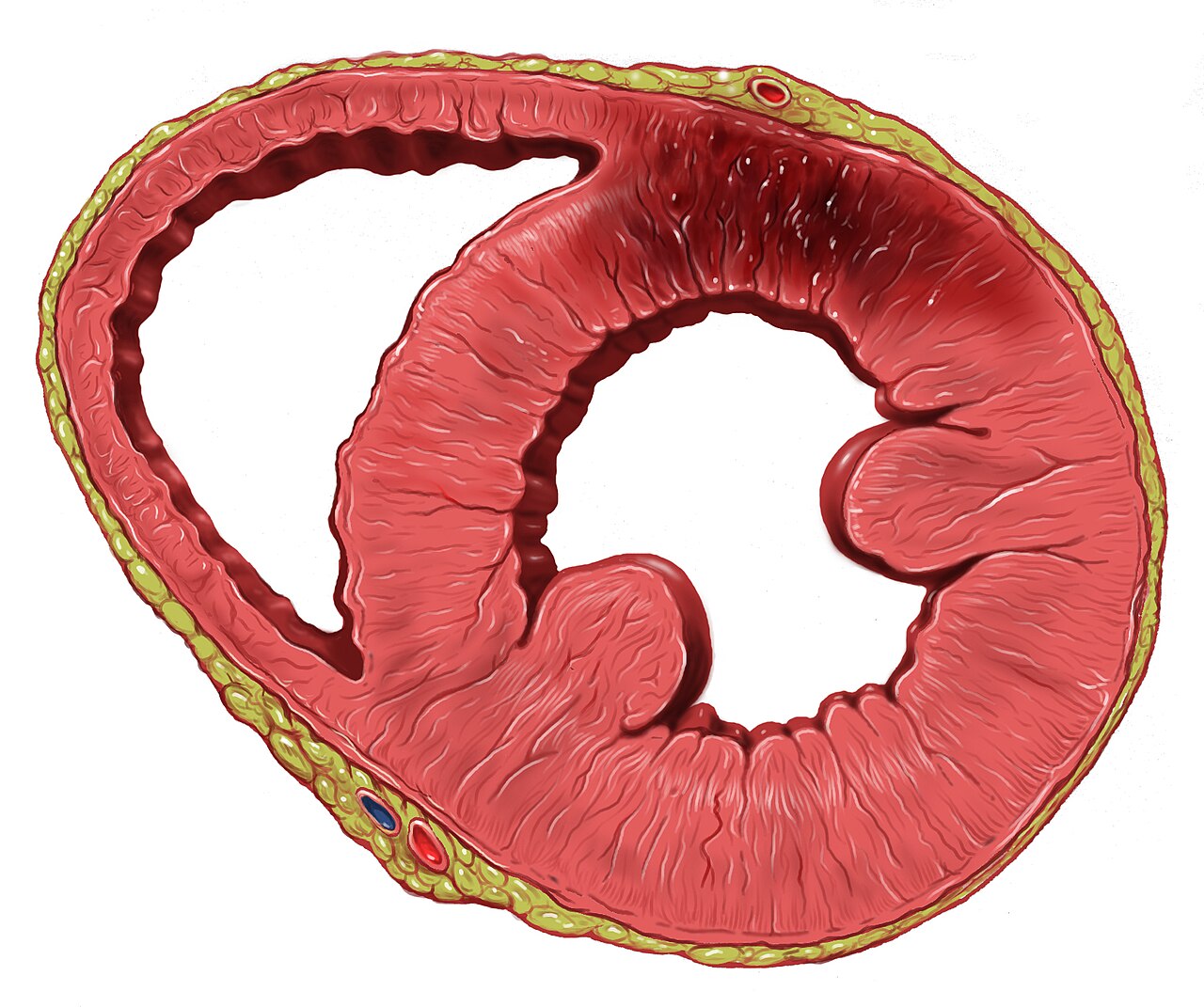
Heart muscle requires a continuous supply of blood and oxygen to function. When a blood vessel that supplies the heart becomes blocked—most commonly by a ruptured atherosclerotic plaque with an overlying clot—the downstream portion of the heart becomes starved of oxygen. This shortage of perfusion is called ischemia. If blood flow is not restored quickly, the ischemic muscle undergoes irreversible injury and infarction (cell death), which is the defining event of myocardial infarction.
Common causes and risk factors
- Atherosclerosis of the coronary arteries leading to plaque rupture and thrombus (clot) formation.
- Coronary artery spasm or persistent narrowing that reduces flow.
- Embolism to a coronary artery in less common situations.
- Major risk factors that increase the chance of MI include smoking, high blood pressure, high cholesterol, diabetes, obesity, a family history of premature heart disease, and physical inactivity.
Symptoms and clinical features
Typical symptoms include pressure, squeezing, or heavy pain in the center of the chest that may radiate to the jaw, neck, shoulder or arm. Shortness of breath, nausea, sweating, lightheadedness and fainting are common. Some people—particularly women, older adults and people with diabetes—experience more subtle symptoms or only fatigue and breathlessness. Episodes of severe ischemic chest pain that do not persist can be termed angina, but prolonged ischemia that causes muscle death is an infarction.
Diagnosis and emergency treatment
Myocardial infarction is a medical emergency. Early evaluation uses an electrocardiogram (ECG) to identify patterns indicating acute injury, and blood tests that detect cardiac enzymes released from damaged muscle. Initial treatment focuses on restoring blood flow and limiting further injury: oxygen if needed, antiplatelet agents, anticoagulants, pain control, and rapid reperfusion by percutaneous coronary intervention (angioplasty and stent) or, when not immediately available, thrombolytic (clot‑dissolving) medication. Rehabilitation and secondary prevention begin during hospital stay and continue after discharge.
Complications, recovery, and prevention
Complications can include heart failure, dangerous heart rhythms, rupture of the heart wall, and formation of aneurysms or clots within the heart. The extent of damage and the speed of treatment influence long‑term outcome. Prevention emphasizes controlling modifiable risks: tobacco cessation, blood pressure and lipid management, glucose control in diabetes, healthy diet, regular exercise, and use of medications when indicated. Public awareness of symptoms and prompt emergency response systems improve survival and reduce disability from myocardial infarction.
Notable distinctions and practical points
- Not all chest pain is a heart attack, but any concerning chest pain should prompt urgent medical assessment.
- Early reperfusion (opening the blocked vessel) is the single most important step to limit permanent damage.
- After an MI, medications such as antiplatelet therapy, statins, beta blockers and ACE inhibitors are commonly used to prevent recurrence and support recovery.
For reliable, detailed guidance on symptoms, emergency response and long‑term care, consult medical resources or health services in your area. Further reading and clinical resources: coronary anatomy, heart structure, circulation basics, oxygen transport, ischemia explanation, angina overview, emergency care.

Epidemiology
Myocardial infarction is one of the main causes of death in industrialized nations. The incidence is about 300 infarctions per 100,000 inhabitants per year in Austria/Germany (in Japan < 100; Mediterranean, Switzerland, France < 200; 300 to 400 in Scandinavia; 400 to 500 in England, Hungary), in Germany about 280,000 people suffer a heart attack every year. According to the cause of death statistics of the Federal Statistical Office, more than 49,000 people died in Germany in 2015 as a result of an acute myocardial infarction. This means that acute myocardial infarction has always ranked second among the causes of death in Germany since 1998. Both the absolute number of deaths as a result of a heart attack and the relative frequency have been steadily declining in Germany for years (see table).
| Year | absolute number | Male | female |
| 2000 | 67.282 | 36.458 | 30.824 |
| 2001 | 65.228 | 35.473 | 29.755 |
| 2002 | 64.218 | 34.907 | 29.311 |
| 2003 | 64.229 | 34.679 | 29.550 |
| 2004 | 61.736 | 33.348 | 28.388 |
| 2005 | 61.056 | 32.973 | 28.083 |
| 2006 | 59.938 | 32.471 | 27.467 |
| 2007 | 57.788 | 31.195 | 26.593 |
| 2008 | 56.775 | 30.559 | 26.216 |
| 2009 | 56.226 | 30.934 | 25.292 |
| 2010 | 55.541 | 30.651 | 24.890 |
| 2011 | 52.113 | 28.621 | 23.492 |
| 2012 | 52.516 | 28.951 | 23.565 |
| 2013 | 52.044 | 28.991 | 23.053 |
| 2014 | 48.181 | 27.188 | 20.993 |
| 2015 | 49.210 | 27.835 | 21.375 |
| 2016 | 48.669 | 28.130 | 20.539 |
| 2017 | 46.966 | 27.130 | 19.836 |
| 2018 | 46.207 | 26.884 | 19.323 |
Heart attacks occur significantly more often in socially poorer neighbourhoods. In addition, in contrast to patients from more socially privileged districts, patients from these neighbourhoods are younger and have a higher risk of dying within one year after the heart attack.

Diagnostics
Current and newer diagnostic methods
The diagnosis of myocardial infarction is made when one of the so-called "biomarkers" (preferably cardiac troponin, alternatively CK-MB) is elevated in the blood and at least one of the following criteria is fulfilled:
- typical ECG changes or
- typical chest pain or
- recent intervention on a coronary vessel (for example, PTCA).
However, the blood concentration of the biomarkers troponin and CK-MB increases only after three to six hours, so that a reliable diagnosis was previously only possible after four to six hours.
According to recent studies, a faster and more specific diagnosis can now be made promptly using the newly discovered cardiac marker glycogen phosphorylase BB (GPBB). GPBB can be used to diagnose a heart attack as early as the first hour, reducing the risk of irreversible damage to heart tissue.
In this acute phase, the most important examination procedure is an ECG obtained as quickly as possible. If ST-segment elevations are detected, an infarction is assumed with a diagnostic certainty of more than 95% and the appropriate treatment is initiated as soon as possible.
If, on the other hand, the ECG shows ST-segment depression or no changes, infarction cannot be excluded or confirmed with certainty on the basis of the biomarkers until six hours after the onset of symptoms. If there is diagnostic uncertainty at this stage, the detection of wall motion abnormality on echocardiography can help to better assess the likelihood and extent of an infarction.
Differential diagnosis
Because of the potentially far-reaching consequences, the suspected diagnosis of myocardial infarction was often made in the past; in the acute situation, the differential diagnoses of pneumothorax, pulmonary embolism, aortic dissection, pulmonary edema of another cause, herpes zoster, stress cardiomyopathy, Roemheld syndrome, cardiac neurosis, or biliary colic then had to be considered. Only about 32% of patients with suspected infarction actually had a heart attack. Today, the term infarction is usually avoided until it is definitively proven, and the term acute coronary syndrome is used instead to reflect the frequent diagnostic uncertainty in the first few hours.
Infarct diagnosis is also subject to possible errors: in some patients (0.8% in one study), especially in elderly patients and those with diabetes mellitus, the infarct is not correctly detected even in hospital.
An unusual confusion of symptoms was observed in a (rather rare) case of consumption of honey from the Turkish Black Sea coast (see Honey#Toxins in honey and toxic honeys).
Questions and answers
Q: What is an acute myocardial infarction?
A: An acute myocardial infarction, also known as a heart attack, occurs when a blood vessel in the heart suddenly becomes blocked and cannot supply enough oxygen to part of the heart.
Q: What is Angina Pectoris?
A: Angina Pectoris is chest pain that results from the lack of oxygen-rich blood in the heart due to an occluded artery.
Q: What does "myocardial infarction" mean?
A: Myocardial infarction means "infarction (muscle death) in the heart muscle."
Q: Is a heart attack a medical emergency?
A: Yes, a heart attack is considered a medical emergency and requires immediate attention.
Q: How long does someone have to get treatment for their heart attack?
A: It is important for someone who has had a heart attack to receive treatment within the first hour of their attack for optimal results.
Q: What happens if there isn't enough oxygen getting to part of the heart?
A: When there isn't enough oxygen getting to part of the heart, it can cause ischemia which can lead to chest pain called Angina Pectoris.
Author
AlegsaOnline.com Myocardial infarction (heart attack): causes, symptoms, and care Leandro Alegsa
URL: https://en.alegsaonline.com/art/67980
Sources
- nhlbi.nih.gov : How is a heart attack treated?
- nlm.nih.gov : Thrombolytic Therapy
- heart.org : Cardiac Catheterization
- nlm.nih.gov : Heart attack first aid