Mast cell: tissue-resident immune cell involved in allergy, defense and repair
Mast cells are tissue-resident leukocytes formed in bone marrow that store histamine and other mediators. They mediate allergic reactions, fight parasites, aid wound healing, and interact with the immune system.
Overview
Mast cells are specialized immune cells that reside in tissues rather than circulating long-term in the blood. They are a type of white blood cell produced from precursors in the bone marrow and mature after they reach skin, mucosa and other tissues. Packed with secretory granules, mast cells are sentinel cells that sense danger, coordinate local defense and influence repair processes.
Image gallery
7 Images




Structure and key components
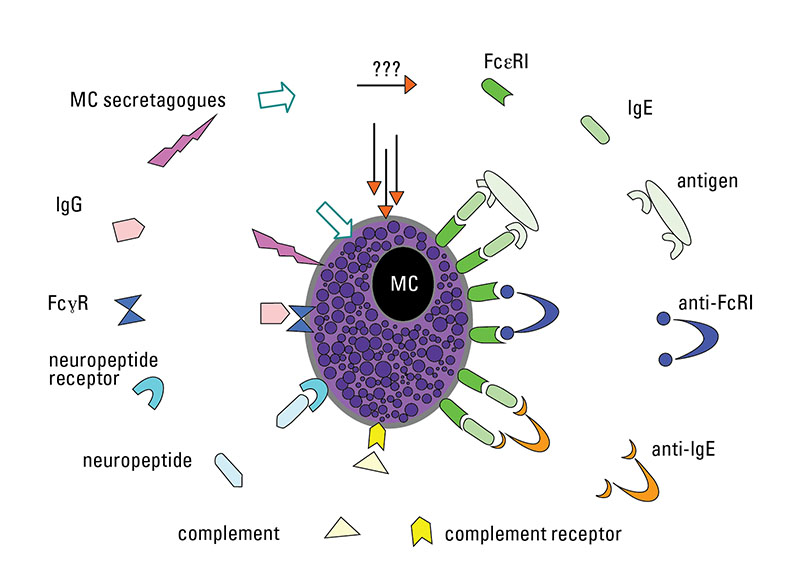
Mast cells contain numerous membrane-bound granules that store preformed mediators such as histamine and heparin, together with proteases (for example tryptase and chymase) and other active molecules. On their surface they express high-affinity IgE receptors (FcéRI) and growth-factor receptors such as c-Kit (CD117), which responds to stem cell factor. When activated, mast cells rapidly release granule contents (degranulation) and also synthesize lipid mediators and cytokines to shape the ensuing inflammatory response.
Functions and clinical importance
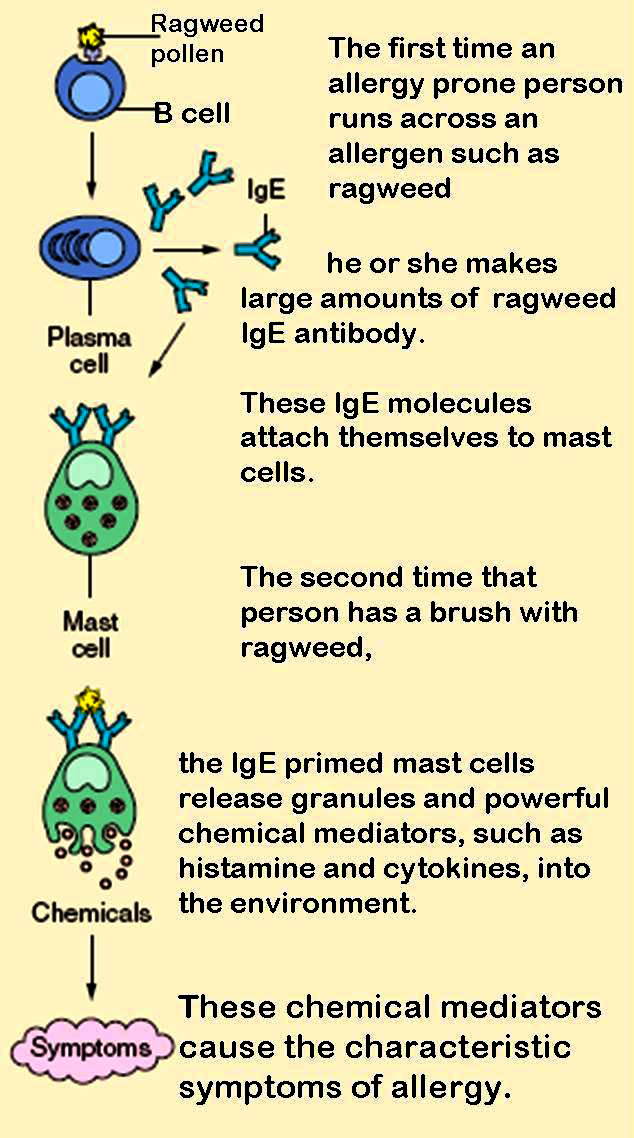
Mast cells play multiple roles in health and disease. They contribute to early defense against parasites and microbes by recruiting other immune cells and by direct antiparasitic mechanisms. They are central to immediate hypersensitivity reactions: IgE-mediated activation of mast cells triggers mediator release that causes symptoms of allergy and, in severe cases, anaphylaxis. Beyond allergy, mast cells participate in wound healing, angiogenesis and tissue remodeling and can influence chronic inflammatory or fibrotic conditions. They also respond to and shape responses against pathogens and interact with T cells, dendritic cells and other immune elements.
Development, classification and distinctions
Mast cells arise from hematopoietic precursors in the bone marrow and complete maturation in peripheral tissues under local signals. Human mast cells are often categorized by their protease content (for example tryptase-only versus tryptase-plus-chymase types), a distinction that relates to tissue localization and function. Superficially similar to blood basophils, mast cells differ by site (tissue-resident versus circulating), life span, receptor repertoire and granule composition, so they are related but distinct cell types within the broader immune system.
History and notable facts
Mast cells were first described in the late 19th century by the German scientist Paul Ehrlich, who noted their prominent granules after staining. The name originally reflected an early interpretation of their appearance. Modern research has since revealed their diverse roles in allergy, host defense and tissue homeostasis, and clinical disorders such as mastocytosis and mast cell activation syndromes are recognized when mast cell number or reactivity becomes pathogenic.
Examples and clinical markers
- Allergic conditions: allergic rhinitis, urticaria and asthma involve mast cell activation.
- Anaphylaxis: systemic mast cell mediator release can cause life‑threatening cardiovascular and respiratory collapse.
- Diagnostics: mediators such as tryptase and histamine are measured to support suspected mast cell activation.
Because mast cells bridge innate and adaptive immunity and influence tissue physiology, they remain a focus of basic research and clinical interest. For more background on foundational concepts, see material about bone marrow, blood cells and inflammatory mediators linked above.

Questions and answers
Q: What is a mast cell?
A: A mast cell is a type of white blood cell that defends against parasites and plays a role in wound healing and defence against pathogens.
Q: Where is a mast cell made?
A: A mast cell is made in bone marrow.
Q: What are some of the granules found in mast cells?
A: Mast cells have granules rich in histamine and heparin.
Q: What is the function of mast cells in wound healing?
A: Mast cells play an important protective role in wound healing.
Q: What is the role of mast cells in defence against pathogens?
A: Mast cells are involved in the defence against pathogens.
Q: What is the connection between mast cells and allergies?
A: Mast cells are a part cause of allergy and anaphylaxis.
Q: Who first described mast cells?
A: Mast cells were first described by Paul Ehrlich in his 1878 doctoral thesis.
Related articles
Author
AlegsaOnline.com Mast cell: tissue-resident immune cell involved in allergy, defense and repair Leandro Alegsa
URL: https://en.alegsaonline.com/art/62720
Sources
- doi.org : 10.1067/mai.2003.120
- pubmed.ncbi.nlm.nih.gov : 12592295