Lassa fever (Lassa haemorrhagic fever)
Acute viral disease endemic in parts of West Africa caused by Lassa virus. Rodent‑borne; most infections are mild but some progress to severe hemorrhagic illness with higher fatality among hospitalized patients.
Overview
Lassa fever, also called Lassa haemorrhagic fever, is an acute viral illness found primarily in parts of West Africa. It is caused by the Lassa virus, a member of the Arenaviridae family. Clinical severity ranges from asymptomatic or mild febrile illness to severe multisystem disease with bleeding, shock and neurological complications. While the majority of infections are not severe, a minority of patients require hospital care and case fatality is higher among those admitted to hospital.
Image gallery
7 Images





Virology and reservoir
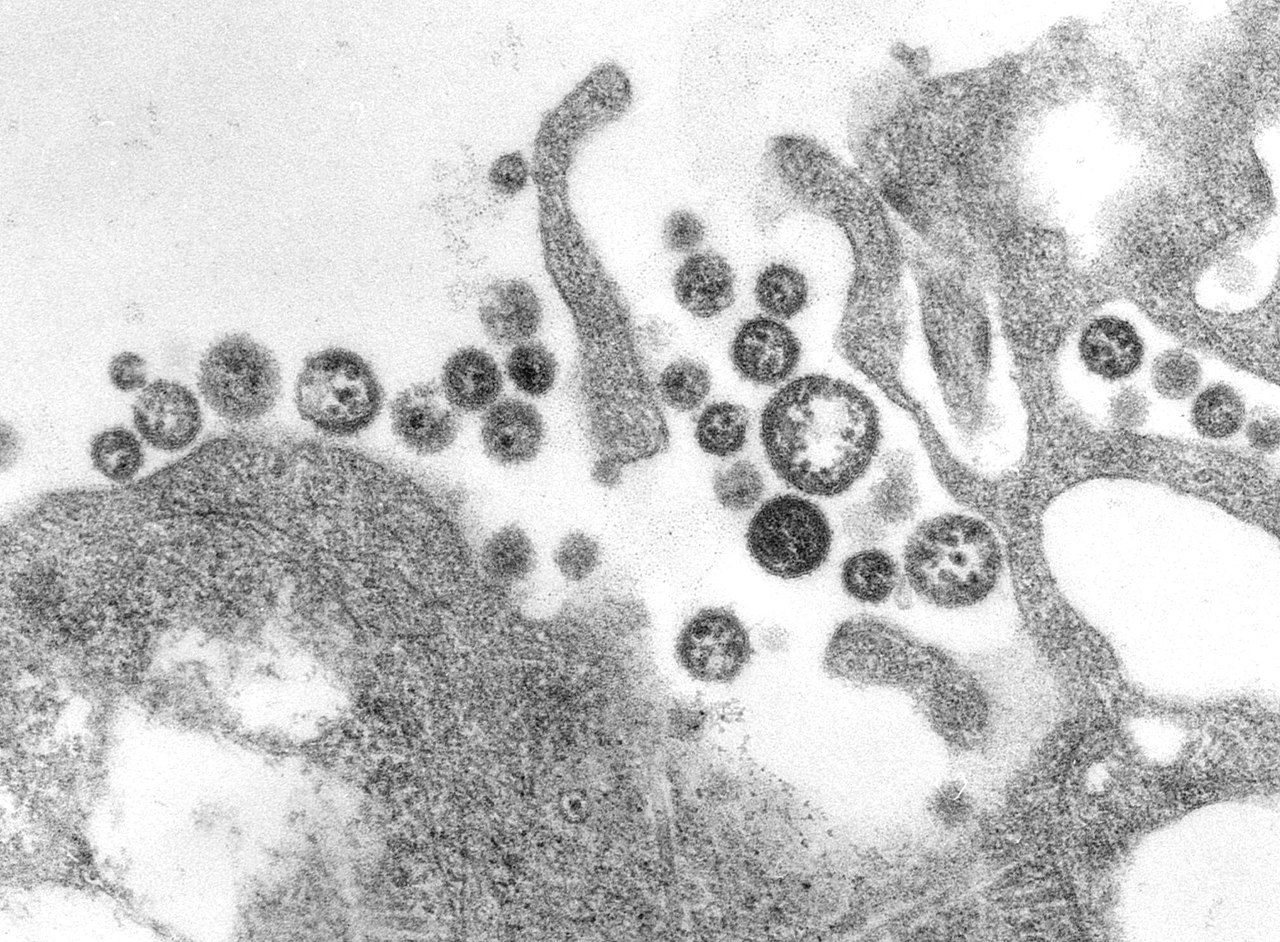
The Lassa virus is a single‑stranded RNA arenavirus. Its principal natural reservoir is the multimammate rat (genus Mastomys), which can harbour and shed the virus in urine and droppings without obvious illness. Humans typically acquire infection by direct or indirect contact with rodent excreta—for example through contaminated food, household items or during agricultural activities.
Transmission and incubation
Transmission is mainly from rodents to people; person‑to‑person spread can occur through contact with blood, secretions or other bodily fluids of an infected person, or through contaminated medical instruments. The incubation period is typically several days to a few weeks. Early symptoms are often non‑specific and may mimic malaria, typhoid or other febrile illnesses, which can delay diagnosis.
Clinical features
- Early signs: fever, malaise, headache, sore throat, muscle aches and gastrointestinal symptoms.
- Progressive disease: persistent vomiting, diarrhoea, facial or neck swelling, bleeding from mucous membranes, respiratory distress and neurological signs in severe cases.
- Risk groups: pregnant women (especially late pregnancy) and those with delayed care have higher risk of severe disease and fatal outcomes.
Diagnosis
Definitive diagnosis relies on laboratory testing performed in appropriately equipped facilities. Common methods include detection of viral RNA by polymerase chain reaction, antigen assays and serology for Lassa‑specific antibodies. Virus isolation is carried out only in high‑containment laboratories. For clinical algorithms and laboratory protocols see available laboratory findings and clinical guides.
Treatment and prognosis
Management is primarily supportive: careful fluid and electrolyte balance, treatment of secondary infections and monitoring for complications. The antiviral drug ribavirin has been used in severe cases and appears most effective when started early. Overall mortality among all infections is lower than among patients who require hospital care; hospitalized case fatality may be substantially higher than in community cases.
Prevention and control
Prevention concentrates on reducing human contact with infected rodents and interrupting person‑to‑person transmission. Key measures include rodent control, safe food storage, improving household hygiene and safe waste management, as well as use of personal protective equipment and strict infection control practices in healthcare settings. Community education and rapid isolation of suspected cases limit spread during outbreaks.
Epidemiology and public health
Lassa fever is endemic in several countries of West Africa, including areas of Nigeria, Liberia, Sierra Leone and Guinea. The disease occurs sporadically and in outbreaks; estimates of total infections vary, and public health authorities emphasise surveillance, laboratory capacity and clinical preparedness to reduce illness and death. Strengthening healthcare systems and community awareness are central to control.
History
The disease was first recognized in 1969 after a cluster of severe cases and the deaths of two nurses drew attention to a novel haemorrhagic illness; early reports linked the events to care of infected patients and led investigators to identify a new virus. The illness was named for the town of Lassa in Borno State, Nigeria, where the index events occurred and where the original cases were described in clinical reports about the nurses involved.
Research and future directions
There is ongoing research into improved diagnostics, antiviral treatments and vaccine candidates. While no widely available licensed vaccine existed as of mid‑2024, several candidates have advanced through early clinical trials. Continued investment in surveillance, rapid diagnostics and clinical care pathways remains a priority for regional and global health agencies.
Questions and answers
Q: What is Lassa fever?
A: Lassa fever is a fever caused by the Lassa virus, which is common in West Africa.
Q: What is the death rate for people who get Lassa fever?
A: One in 80 people who get Lassa fever will die.
Q: Are all cases of Lassa fever severe?
A: No, not all cases of Lassa fever are severe. Some cases require going to a hospital, while others do not.
Q: What is the death rate for severe cases of Lassa fever?
A: The death rate for severe cases of Lassa fever is 1 in 5.
Q: When was Lassa Fever discovered?
A: Lassa Fever was discovered in 1969.
Q: Why was Lassa Fever named as such?
A: Lassa Fever was named for the town in Borno State, Nigeria where it was first diagnosed.
Q: How did the discovery of Lassa Fever come about?
A: The discovery of Lassa Fever came about after two nurses died from the disease.
Related articles
Author
AlegsaOnline.com Lassa fever (Lassa haemorrhagic fever) Leandro Alegsa
URL: https://en.alegsaonline.com/art/56136
Sources
- pubmed.ncbi.nlm.nih.gov : 17378212
- cdc.gov : "Lassa Fever"
- ncc.gov.ng : "The Facts on Lassa Fever"