Kwashiorkor: severe protein malnutrition affecting young children
Kwashiorkor is a form of severe malnutrition caused primarily by inadequate dietary protein, leading to edema, growth failure, liver changes and increased infection risk, most often in young children.
Overview
Kwashiorkor is a clinical syndrome of severe protein deficiency that occurs most commonly in young children after the period of breastfeeding ends. It is one form of protein–energy malnutrition distinguished by prominent swelling (edema) and changes in the skin, hair and liver. The disorder typically appears where diets provide sufficient calories from starches but are low in high-quality protein, often in contexts of poverty, food insecurity or famine. For a general introduction see nutrition overview.
Image gallery
1 Image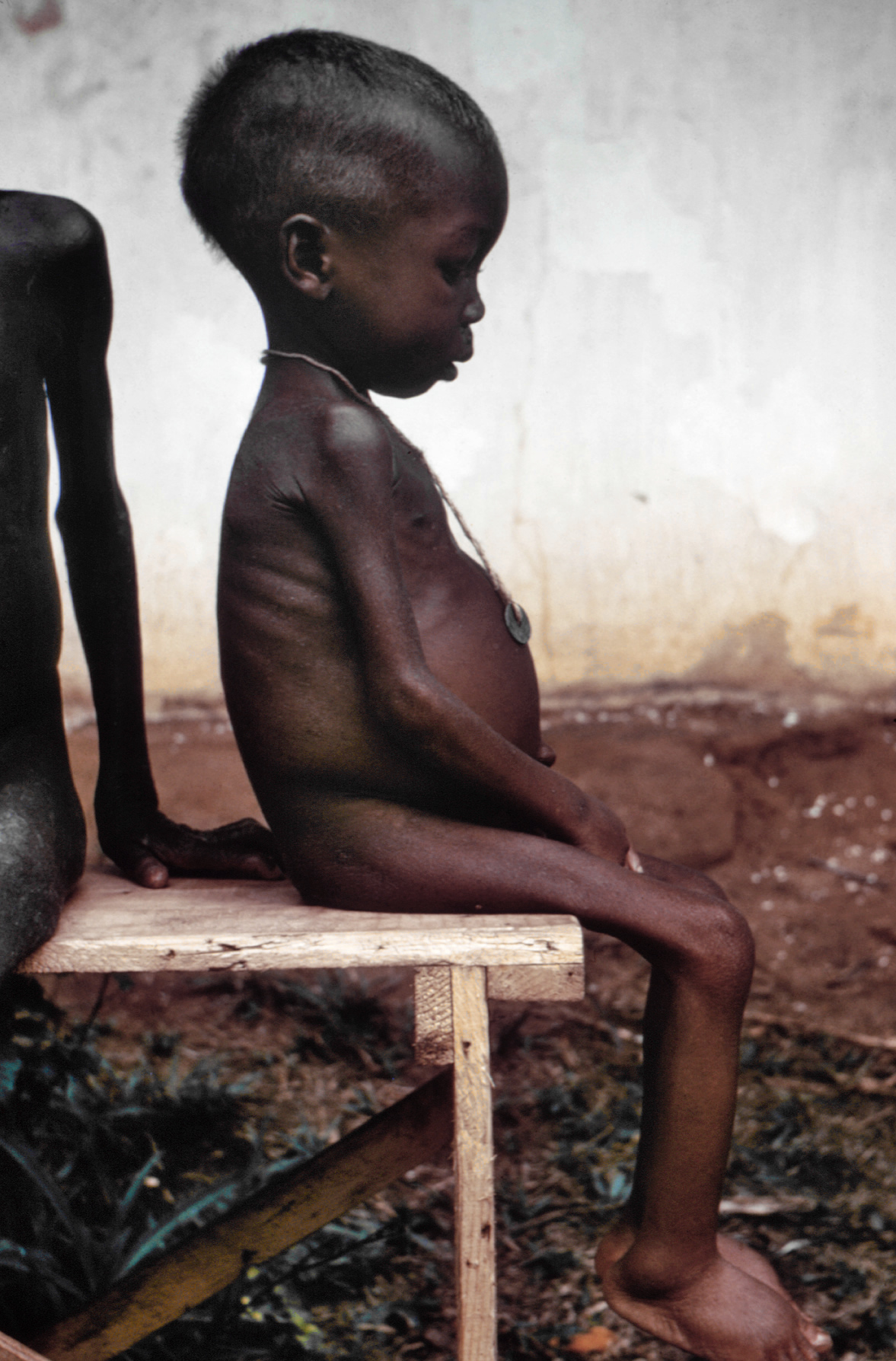
Key characteristics and signs
Typical features include generalized pitting edema (swelling of the feet, legs and face), a distended abdomen, thin wasted muscles, irritability, loss of appetite and slow or halted linear growth. The hair may become thin and change color, and the skin can develop scaly or ulcerating lesions. Many affected children also show enlarged, fatty liver and laboratory signs such as low serum proteins. Secondary infections, diarrhea and poor wound healing are common complications. For descriptions of clinical signs consult protein deficiency resources and energy metabolism references.
Causes and biological mechanisms
Kwashiorkor arises when dietary protein is inadequate relative to the body's needs, especially during growth. Low levels of circulating proteins — notably albumin — reduce the osmotic pressure that normally keeps fluid within blood vessels, contributing to edema. Other proposed mechanisms include impaired antioxidant defenses, disrupted gut integrity, micronutrient deficiencies and altered liver function leading to fat accumulation. The condition reflects a complex metabolic response to insufficient amino acids rather than a simple shortage of calories alone. Further reading on metabolic aspects is available at metabolism and nutrition.
History, epidemiology and risk factors
The term "kwashiorkor" was coined in the mid-20th century to describe a syndrome noted in formerly breastfed children after weaning. It remains associated with regions facing chronic undernutrition and limited dietary diversity, including parts of sub-Saharan Africa, South Asia and areas experiencing humanitarian crises. Risk factors include early weaning, diets heavily based on starchy staples, recurrent infections and poverty. Public health and maternal-child programs aim to reduce incidence through improved feeding practices and food security.
Treatment, recovery and prevention
Management begins with careful medical stabilization: treating dehydration and infections, correcting electrolyte and micronutrient imbalances, and introducing therapeutic feeding that gradually restores energy and protein while monitoring for refeeding complications. Recovery can be prolonged; some children regain weight but may have lasting developmental delays. Preventive strategies emphasize breastfeeding, timely introduction of nutrient-dense complementary foods, community nutrition programs and food assistance where needed. For clinical guidance and patient resources see clinical nutrition guidance and advice on managing complications at infection and diarrhea resources.
Distinguishing note: Kwashiorkor differs from marasmus, another form of severe malnutrition characterized mainly by wasting without the prominent edema seen in kwashiorkor; mixed forms may also occur. Understanding these distinctions helps guide appropriate care and public health responses.
Questions and answers
Q: What is Kwashiorkor?
A: Kwashiorkor is a health condition caused by a lack of protein in the diet, leading to poor nutrition.
Q: What happens if a person uses up energy from carbohydrates and lipids?
A: If a person uses up energy from carbohydrates and lipids, their body may begin to use protein for energy instead, leading to a protein deficiency.
Q: Who is most at risk of getting Kwashiorkor?
A: Kwashiorkor is most common in children aged 1 to 5 years old, especially in poor areas of Africa. However, it can rarely affect adults and older children as well.
Q: What are the symptoms of Kwashiorkor?
A: Symptoms of Kwashiorkor include having a pot belly, a swollen face, hair that is dark then light then dark, poor muscle development, swollen legs, a puffy face, difficulty in eating, diarrhea, and dry skin.
Q: How can Kwashiorkor be treated?
A: Kwashiorkor can be treated by having a protein-rich diet to address the protein deficiency.
Q: What happens to the body during Kwashiorkor?
A: During Kwashiorkor, body parts become swollen due to an accumulation of water in the spaces between the body's cells.
Q: What bodily functions are affected by Kwashiorkor?
A: Kwashiorkor can affect bodily functions such as growth and tissue building, as the body does not have enough protein for these processes.
Related articles
Author
AlegsaOnline.com Kwashiorkor: severe protein malnutrition affecting young children Leandro Alegsa
URL: https://en.alegsaonline.com/art/54735