Apgar score: quick assessment of a newborn's immediate condition
Concise encyclopedia entry on the Apgar score: origin, five components, scoring, timing, interpretation, uses, limits, and special situations in newborn assessment.
Overview
The Apgar score is a rapid, standardized method for assessing the clinical condition of a newborn immediately after birth. Devised in 1952 by anesthesiologist Virginia Apgar, it provides a short bedside snapshot used to identify infants who need urgent assistance and to document initial status. Because it is quick and requires no equipment, the Apgar score remains widely used in delivery rooms, by midwives, obstetric and neonatal teams, and emergency providers. For practical clinical pathways and summaries see clinical guidance.
Image gallery
2 Images
Components and scoring
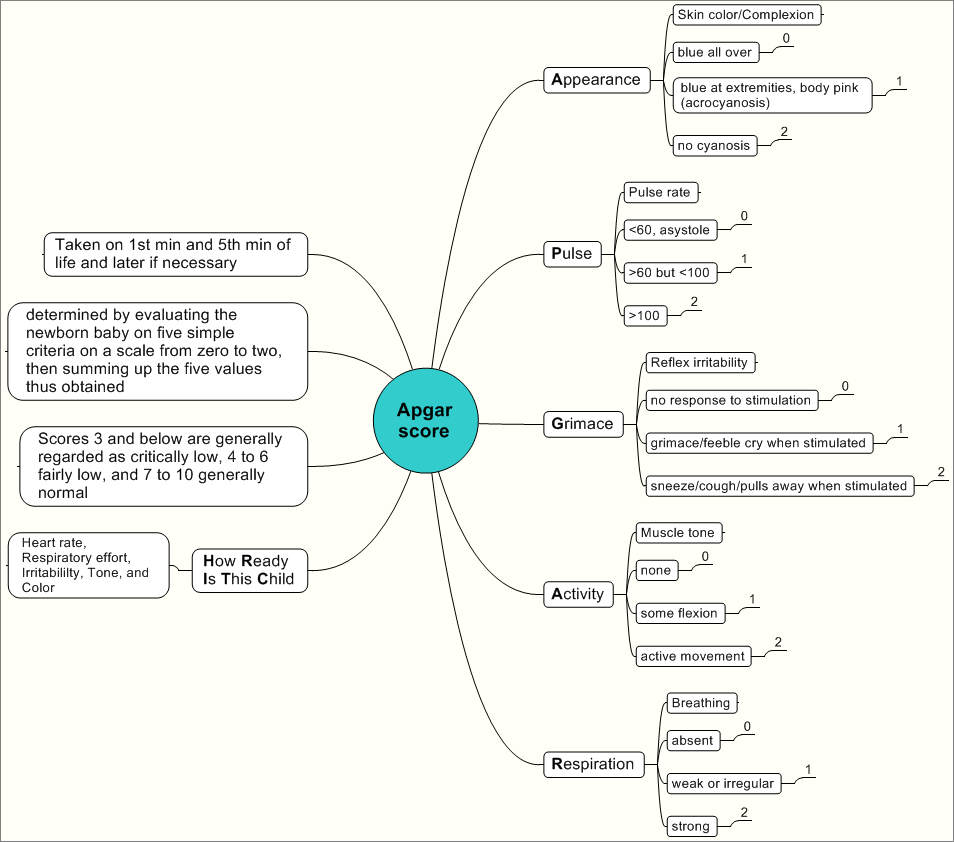
The assessment covers five signs. Each sign is scored 0, 1, or 2; the total ranges from 0 to 10. The mnemonic APGAR (Appearance, Pulse, Grimace, Activity, Respiration) is commonly used to remember the components. Typical scoring criteria are:
- Appearance (color): 0 = pale or blue all over; 1 = body pink, extremities blue (acrocyanosis); 2 = entirely pink.
- Pulse (heart rate): 0 = absent; 1 = <100 beats per minute; 2 = ≥100 beats per minute.
- Grimace (reflex irritability): 0 = no response to stimulation; 1 = grimace or weak response to stimulation; 2 = vigorous response such as coughing, sneezing, or pulling away.
- Activity (muscle tone): 0 = limp; 1 = some flexion of arms and legs; 2 = active motion.
- Respiration: 0 = absent; 1 = slow or irregular breaths; 2 = good, strong cry or regular breathing effort.
Timing and how scores are used
Standard practice is to record Apgar scores at 1 minute and 5 minutes after birth. If the 5‑minute score is low, additional scores (for example at 10 minutes) are often recorded to monitor progress. Scores of 7–10 at 5 minutes are generally considered reassuring; scores below 7 indicate the infant may need medical support such as stimulation, airway clearance, supplemental oxygen, or more active resuscitation. Very low initial scores (for example ≤3) usually prompt immediate intervention and closer monitoring. For protocols on neonatal resuscitation consult resuscitation resources and local practice recommendations.
Interpretation, strengths and limitations
The Apgar score is valuable because it is simple, quick, and reproducible for documenting immediate condition and the need for resuscitation. However, it has important limitations. It was not designed to predict long‑term neurological outcome, and single low scores should not be taken as definitive prognostic indicators. Scores can be influenced by prematurity, maternal medications, congenital anomalies, infections, fetal blood loss, and the infant's transition physiology. Interobserver variation is possible; training and consistent scoring practice improve reliability. For an in‑depth review of limitations and evidence see detailed review.
Special situations
Some clinical situations affect Apgar interpretation. Preterm infants often have lower scores because of immature muscle tone and respiration, even when not acutely ill. Cesarean delivery, maternal general anesthesia, and opiate exposure during labor can depress respiration and tone transiently. When resuscitation measures (such as positive‑pressure ventilation or intubation) are in place, documentation should note the interventions because they influence the score and clinical context. In medicolegal or research settings, the score should be interpreted alongside other clinical data, including cord blood gas values and ongoing neonatal assessments.
Use in practice and research
Clinically, the Apgar score guides immediate resuscitation decisions and helps communicate condition among care teams. In public health and research it is used as a simple marker for population surveillance and epidemiologic studies of perinatal outcomes, with the caveat that it is a crude indicator and should be combined with other measures when evaluating long‑term development or causation. Modified approaches or additional assessments are recommended when more precise physiologic information is needed.
History and legacy
Virginia Apgar developed the score to provide a uniform, rapid assessment to evaluate the effects of obstetric anesthesia and improve newborn care. Over decades the Apgar score has become an enduring part of delivery‑room practice worldwide. It is taught in basic neonatal training and incorporated into newborn charts, while modern neonatal care also relies on monitoring, blood gas analysis, and structured resuscitation algorithms. For historical context and biographical material see historical sources and biographical material.
Practical tips
- Score at exactly 1 and 5 minutes and record whether interventions were performed when scoring.
- Train staff to apply criteria consistently and to recognize when additional monitoring or referral is required.
- Use the Apgar score together with clinical judgment and other measurements rather than as a sole determinant of prognosis.
Note: This entry summarizes widely accepted uses and limits of the Apgar score; it is not a substitute for clinical protocols or local guidelines.
Questions and answers
Q: What is the Apgar score?
A: The Apgar score is a quick way of measuring how healthy a newborn baby is.
Q: Who invented the Apgar score and why?
A: Virginia Apgar, an anesthesiologist, invented the Apgar score in 1952 to measure how babies were affected by anesthesia given to their mothers during childbirth.
Q: Who uses the Apgar score?
A: The Apgar score is commonly used by doctors, nurses, midwives, emergency medical technicians (EMTs), and other medical professionals.
Q: Why is the Apgar score so popular?
A: One of the reasons the Apgar score is so popular is that it is very quick to perform, usually taking less than a minute.
Q: What five simple things about the newborn are checked during an Apgar test?
A: During an Apgar test, the five simple things that are checked about the newborn are Appearance, Pulse, Grimace, Activity, and Respiration.
Q: How are scores assigned during an Apgar test?
A: The newborn gets a score of 0, 1, or 2 on each of the five things checked during an Apgar test, and the scores are added up to determine the newborn's Apgar score.
Q: What does the word "APGAR" stand for?
A: "APGAR" is a backronym that stands for the five things the Apgar scale checks: Appearance, Pulse, Grimace, Activity, and Respiration.
Related articles
Author
AlegsaOnline.com Apgar score: quick assessment of a newborn's immediate condition Leandro Alegsa
URL: https://en.alegsaonline.com/art/4869
Sources
- apgar.net : "A proposal for a new method of evaluation of the newborn infant"
- doi.org : 10.1213/00000539-195301000-00041
- pubmed.ncbi.nlm.nih.gov : 13083014
- doi.org : 10.1097/00000542-200504000-00022
- pubmed.ncbi.nlm.nih.gov : 15791116
- acog.org : "Committee Opinion Number 644: The Apgar Score"
- doi.org : 10.1056/NEJM200102153440701
- pubmed.ncbi.nlm.nih.gov : 11172187