Intervertebral disc
Soft fibrocartilaginous pads between vertebrae that absorb shock, permit limited spinal motion and maintain spacing; composed of annulus fibrosus and nucleus pulposus and central to common back disorders.
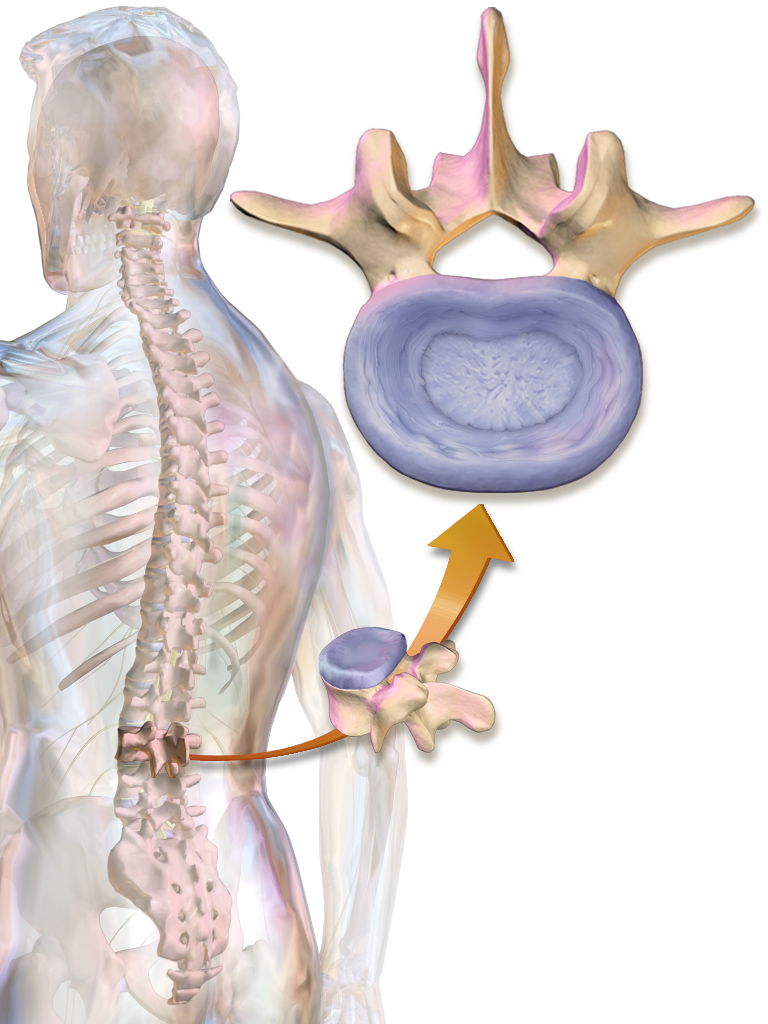
The intervertebral disc is a soft, fibrocartilaginous structure positioned between adjacent vertebrae along the human spine. It forms part of the functional unit that links adjacent bones while permitting small amounts of movement and helping to distribute mechanical loads. In anatomical terms the disc is a fibrocartilaginous element and contributes to the overall stability of the spinal column as a connective tissue that also functions like a ligament.
Image gallery
10 Images






Structure and composition
Each disc typically has two principal components: an outer ring called the annulus fibrosus and a central, gel-like core called the nucleus pulposus. The annulus fibrosus consists of concentric layers of collagen fibers with both type I and type II collagen; type I is concentrated at the periphery to provide tensile strength. The nucleus pulposus is rich in proteoglycans and water, containing loose collagen fibers suspended within a mucous matrix reminiscent of a mucoprotein gel. Thin cartilaginous endplates connect the disc to the adjacent vertebral bodies and help transmit nutrients into the largely avascular disc tissue.
Functions and biomechanics
Discs act primarily as shock absorbers and spacing elements. Under load the nucleus pulposus behaves hydrostatically: pressure spreads radially and is borne by the annulus fibrosus. This arrangement evens out forces across the vertebral endplates, reduces point loading, and allows the spine to flex, extend, bend and rotate a little between each pair of vertebrae. By maintaining disc height the structure also preserves the size of intervertebral foramina through which spinal nerves pass.
Development, aging and variation
During embryonic development the nucleus pulposus originates from remnants of the embryonic notochord, while surrounding mesenchymal tissue forms the annulus and endplates. With age the disc tends to lose water and proteoglycan content, becoming stiffer and less able to absorb shocks; fissures or clefts may form in the annulus and disc height often diminishes. Disc size and shape vary along the spine—cervical discs are smaller and allow more mobility whereas lumbar discs are larger and bear greater loads.
Clinical significance and common conditions
Intervertebral discs are central to many spinal disorders. Degenerative disc disease, disc bulge, and disc herniation are frequent causes of back and neck pain and may compress nearby nerve roots, producing radicular symptoms. Diagnosis commonly uses imaging, clinical examination and sometimes electrophysiological tests. Treatments range from conservative measures—physical therapy, analgesics and injections—to surgical options such as discectomy, spinal fusion or artificial disc replacement depending on severity and patient factors. The disc’s role as a load-bearing and motion-allowing structure makes it a frequent focus in spine care and ergonomics.
Key distinctions and notable facts
- The annulus fibrosus provides tensile strength; the nucleus pulposus provides compressive resistance via hydrostatic pressure.
- Intervertebral discs are essentially avascular after early childhood; nutrition occurs by diffusion through endplates.
- Pathology is influenced by genetics, mechanical load, smoking and systemic health; not all degenerative changes cause pain.
- Discs form part of a functional spinal unit sometimes described as a small joint complex together with the facet joints.
For readers seeking more detailed anatomy, biomechanics or treatment options, see specialized references and clinical guidelines available through professional sources and anatomy texts (vertebrae, spine, fibrocartilaginous).
Questions and answers
Q: What is an intervertebral disc?
A: An intervertebral disc is a kind of padding between vertebrae in the vertebral column.
Q: What is the importance of an intervertebral disc?
A: Intervertebral discs are shock absorbers in the spine and are very important to the health of the spine.
Q: What type of joint is the fibrocartilaginous disc?
A: The fibrocartilaginous disc is a joint.
Q: What is the composition of the outer fibrous ring of an intervertebral disc?
A: The outer fibrous ring of an intervertebral disc is made up of both type I and type II collagen.
Q: What is the nucleus pulposus and what is its function?
A: The nucleus pulposus is a component of the intervertebral disc that contains loose fibers suspended in a mucoprotein gel. It helps to distribute pressure evenly across the disc and acts as a shock absorber, keeping the two vertebrae separated.
Q: Where is type I collagen concentrated in the fibrous outer ring of the intervertebral disc?
A: Type I collagen is concentrated towards the edge of the fibrous outer ring where it provides greater strength.
Q: What is the origin of the nucleus pulposus?
A: The nucleus pulposus is the remnant of the notochord.
Author
AlegsaOnline.com Intervertebral disc Leandro Alegsa
URL: https://en.alegsaonline.com/art/47849
Sources
- doi.org : 10.1242/dmm.008128