Human papillomavirus (HPV): causes, types, prevention and treatment
Comprehensive overview of human papillomavirus (HPV): biology, transmission, disease spectrum, screening and vaccines, plus common treatments and public health importance.
Overview
Human papillomavirus (HPV) is a large family of DNA viruses that infect the skin and mucous membranes of humans. More than 100 distinct HPV types have been identified. Most infections cause no symptoms and are cleared by the immune system, but some types produce visible benign growths called warts, while a subset—known as high‑risk or oncogenic types—can persist and lead to precancerous lesions and invasive cancer.
Image gallery
8 Images






Characteristics and types
HPV types are often grouped by the tissues they infect and the disease risk they carry. About 40 types infect the anogenital tract and can be sexually transmitted; roughly 12–15 of those are classed as high‑risk for causing cancer. Well known high‑risk types include HPV‑16 and HPV‑18, which are responsible for a large share of HPV‑related malignancies. Other types tend to cause common skin warts or plantar warts. Infection can affect the external genitalia, the cervix, the oral cavity and the oropharynx (inside the mouth and throat), among other sites.
Transmission and natural history
HPV spreads primarily through direct skin‑to‑skin contact. Sexual contact is the main route for anogenital and oral infections, but any contact between infected and susceptible epithelium can transmit the virus. Condoms reduce but do not completely eliminate transmission because HPV may infect areas not covered by a condom. In most people the immune response clears HPV within months to a couple of years; persistent infection with high‑risk types is the key factor that can progress to precancerous changes and cancer over many years.
Clinical manifestations and diagnosis
Clinical outcomes vary by HPV type and site of infection. Typical manifestations include:
- Common warts on hands and feet, and genital warts in the anogenital region.
- Precancerous lesions of the cervix, vulva, vagina, penis, anus or oropharynx.
- Invasive cancers, most notably cervical cancer, and an increasing proportion of oropharyngeal cancers.
Screening programs—such as cytologic testing (Pap smears) and HPV DNA tests for cervical disease—detect abnormalities early so they can be monitored or treated before progression. Diagnosis of warts is usually clinical, though laboratory typing is available when needed.
Prevention
Primary prevention focuses on vaccination and safer sexual practices. Licensed prophylactic HPV vaccines protect against the most common high‑risk types and the types that cause most genital warts; they are most effective when given before first exposure to the virus. Secondary prevention includes organized cervical screening for early detection of precancerous changes in the cervix (cervical screening).
Treatment
Treatment depends on the lesion type and location. For external warts, first‑line, over‑the‑counter options include topical agents such as salicylic acid, which is widely sold in pharmacies. Clinically resistant warts may be treated by professional methods: cryotherapy (freezing), surgical removal, electrosurgery, or ablation with a laser. Persistent or high‑grade precancerous cervical lesions are managed by excisional or ablative procedures to remove abnormal tissue; more advanced cancers require oncologic treatment, which can include radiation, surgery and systemic therapies. In specialized settings, topical immunomodulators and other medical treatments are also used; when cancer requires systemic control, various forms of chemotherapy may be part of care.
Public health and notable facts
HPV is one of the most common human viral infections and a major, preventable cause of cancer worldwide. Vaccination programs and screening have substantially reduced precancerous disease in populations with high coverage. Education, vaccination of adolescents, and continued screening remain central strategies for lowering the burden of HPV‑associated disease. For further background and clinical guidance, consult public health resources and professional medical sources provided by health authorities and specialists (virus overview, vaccine information).
Virus Groups
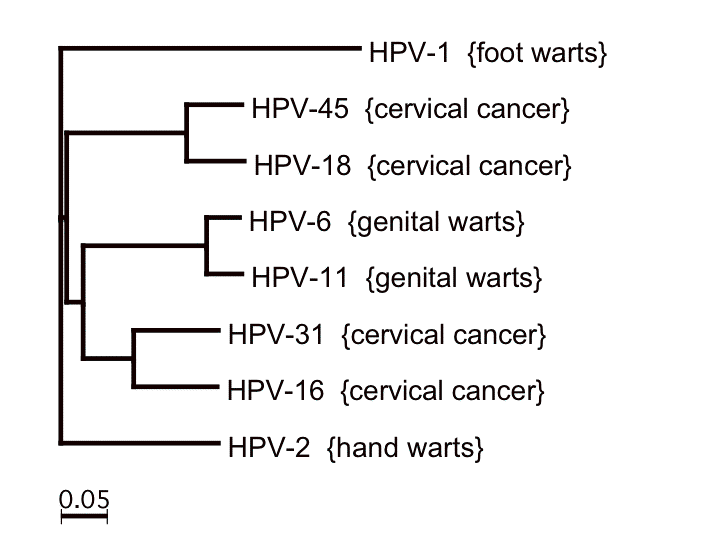
A distinction must be made between classification (based on the clinical picture and course of the disease) and taxonomy (based on genetic relationship).
Classification
To date, 124 HPV types have been fully described. About 30 of them almost exclusively infect the skin and mucosa in the anogenital region (anus and genitals). The genital HPV types can generally be divided into two groups, the low-risk and the high-risk types. The classification is based on the risk type: a few pathogens occur extremely frequently in connection with carcinomas.
- The high-risk types have been identified in 99.7 % of all cases of cervical carcinoma (cancerous tumours of the cervix). In turn, the majority of cervical carcinomas (about 70%) are caused by high-risk types 16 and 18, followed by genotypes 31 and 33.
- The low-risk types are almost never directly involved in the development of cervical carcinoma. In the case of multiple infections (infections with more than one HPV genotype), however, they can also be detected in cervical carcinomas, but then together with a clinically relevant high-risk type.
The guys are:
- "low-risk viruses
HPV 6 and 11 are included in this group because, as the main causes of warts in the genital area (condylomata acuminata, also known as "genital warts"), they are not potentially life-threatening pathogens. Other low-risk types are 40, 42, 43, 44, 54, 61, 70, 72, 81 and CP6108.
- "high-risk viruses
The second group mainly includes HPV 16, 18, 31 and 33, but also 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82. In almost every case of cervical carcinoma (cancer of the epithelial tissue of the cervix), at least one of the high-risk HPV groups is detectable in HPV screening. Some cancers of the anus and mouth are also considered HPV-associated.
- possibly "high-risk" viruses
These include HPV 26, 53 and 66.
- Viruses without clear risk assignment (HPV genotypes of undetermined risk)
In 2005, the IARC officially classified genotypes 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 66 as carcinogenic. The dangerous virus subgroups have been shown to be involved not only in the development of cervical cancer, but are also found in cancers of the penis, vulva (external female genitalia), anus and throat.
System
The decision on different taxa (taxonomic, i.e. relationship groups) is deliberated and made by an international body, the International Committee on Taxonomy of Viruses (ICTV). As of November 2018, the taxonomy of the Papillomaviridae is as follows (for genera with only a single species, the species is numbered 1 and is not specifically listed):
· Family Papillomaviridae
· Subfamily Firstpapillomavirinae
· Genus Alphapapillomavirus (with species Alphapapillomavirus 1 to 14)
· Genus Betapapillomavirus (with species Betapapillomavirus 1 to 6)
· Genus Gammapapillomavirus (with species Gammapapillomavirus 1 to 27)
· Genus Deltapapillomavirus (with species Deltapapillomavirus 1 to 7)
· Genus Epsilon papillomavirus (with species Epsilon papillomavirus 1 and 2)
· Genus Zetapapillomavirus
· Genus Etapapillomavirus
· Genus Thetapapillomavirus
· Genus Iotapapillomavirus (including species Iotapapillomavirus 1 and 2)
· Genus Kappapapillomavirus (with species Kappapapillomavirus 1 and 2)
· Genus Lambdapapillomavirus (with species Lambdapapillomavirus 1 to 5)
· Genus Mupapillomavirus (with species Mupapillomavirus 1 to 3)
· Genus Nupapillomavirus
· Genus Xipapillomavirus (with species Xipapillomavirus 1 to 5)
· Genus Omicron papillomavirus
· Genus Chipapillomavirus (with species Chipapillomavirus 1 to 3)
· Genus Pipapillomavirus (with species Pipapillomavirus 1 and 2)
· Genus Rhopapillomavirus (with species Rhopapillomavirus 1 and 2)
· Genus Sigmapapillomavirus
· Genus Taupapillomavirus (with species Taupapillomavirus 1 to 3)
· Genus Upsilon papillomavirus (with species Upsilon papillomavirus 1 to 3)
· Genus Phipapillomavirus
· Genus Psipapillomavirus (with species Psipapillomavirus 1 to 3)
· Genus Omegapapillomavirus
· Genus Dyodeltapapillomavirus
· Genus Dyoepsilon papillomavirus
· Genus Dyozetapapillomavirus
· Genus Dyoetapapillomavirus
· Genus Dyothetapapillomavirus
· Genus Dyoiotapapillomavirus (including species Dyoiotapapillomavirus 1 and 2)
· Genus Dyocappapillomavirus (with species Dyocappapillomavirus 1 to 5)
· Genus Dyolambdapapillomavirus
· Genus Dyomupapillomavirus
· Genus Dyonupapillomavirus
· Genus Dyoxipapillomavirus (with species Dyoxipapillomavirus 1 and 2)
· Genus Dyoomicron papillomavirus
· Genus Dyopipapillomavirus
· Genus Dyorhopapillomavirus
· Genus Dyosigmapapillomavirus
· Genus Dyotaupapillomavirus
· Genus Dyophipapillomavirus
· Genus Dyoupsilon papillomavirus
· Genus Dyopsipapillomavirus
· Genus Dyoomegapillomavirus
· Genus Treisdeltapapillomavirus
· Genus Treisepsilon papillomavirus
· Genus Treiszetapillomavirus
· Genus Treisetapapillomavirus
· Genus Treisthetapapillomavirus
· Genus Treisiotapapillomavirus
· Genus Treiskappapillomavirus
· Subfamily Secondpapillomavirinae
· Genus Alefpapillomavirus
Transmission
The infection occurs mainly through skin contact, and for certain virus types primarily through unprotected sexual intercourse (genital, anal or oral sex). The HPV infection is therefore one of the most common infections transmitted through sexual intercourse, but often the infection goes unnoticed. Condoms can halve the risk of infection. More rarely, the viruses are also transmitted through shared towels, drinking glasses or toothbrushes. In the context of an already existing infection, pubic hair removal by shaving can lead to infection of previously unaffected areas of the body.
Related articles
Author
AlegsaOnline.com Human papillomavirus (HPV): causes, types, prevention and treatment Leandro Alegsa
URL: https://en.alegsaonline.com/art/45658
Sources
- cancer.gov : HPV vaccine fact sheet
- cancer.gov : HPV fact sheet
- oralcancerfoundation.org : HPV oral cancer facts