Herpes simplex: causes, symptoms, transmission, and management
Herpes simplex (HSV) is a common viral infection causing oral and genital lesions. This article explains types, symptoms, latency, diagnosis, treatment, prevention, complications, and key distinctions.
Overview
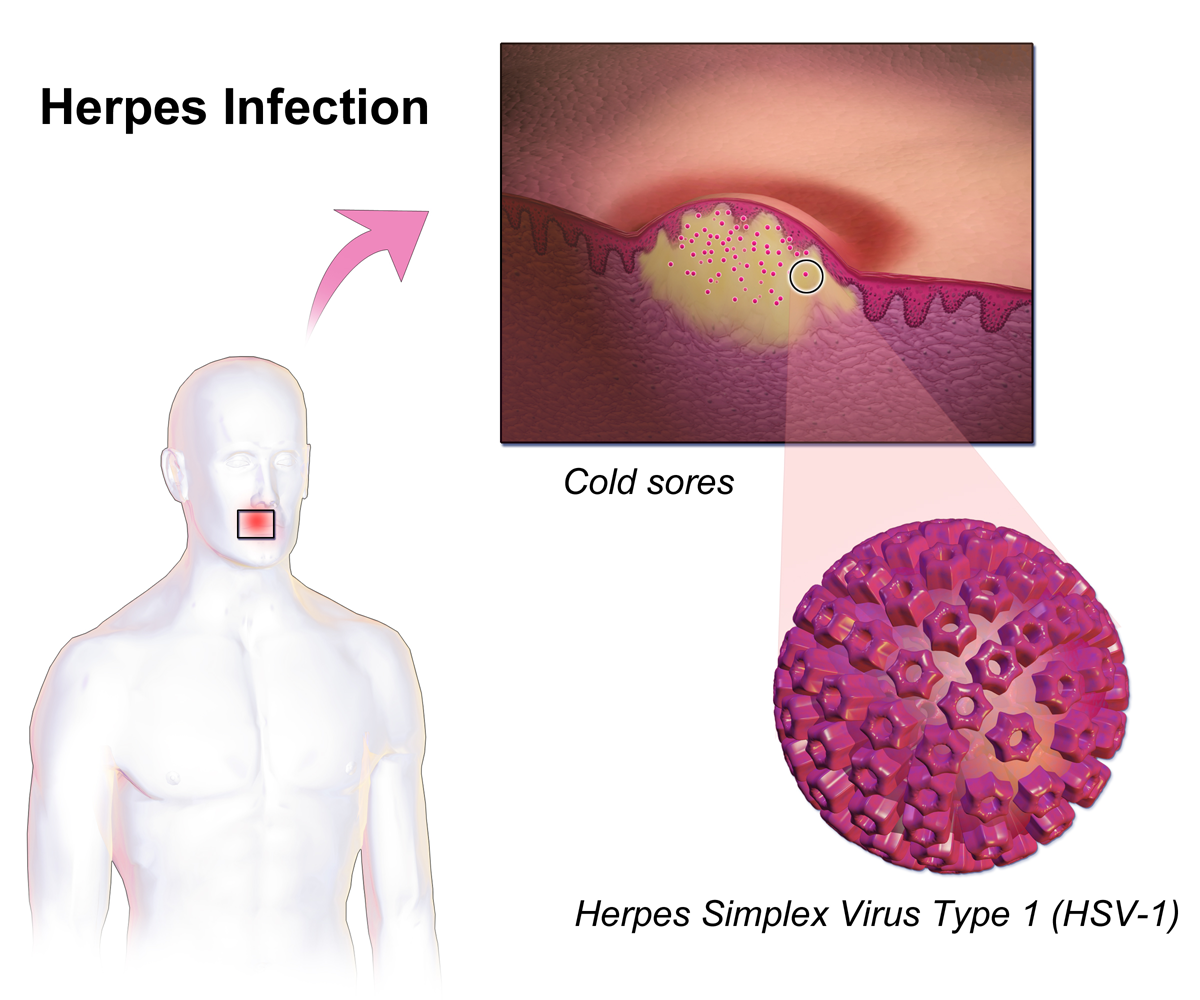
Herpes simplex refers to infections caused by herpes simplex viruses (HSV), members of the Herpesviridae family. Two principal types, HSV-1 and HSV-2, cause painful, fluid-filled blisters on skin or mucous membranes, most commonly around the mouth (oral) or the genitals. Infections are widespread worldwide and may be symptomatic or entirely unnoticed. Once a person becomes infected the virus establishes lifelong latency and can reactivate intermittently.
Image gallery
10 Images







Signs, course and clinical manifestations
Primary infection may produce fever, malaise and clusters of blisters that break into shallow ulcers and crust over. After healing the virus remains dormant in sensory nerve ganglia and can reactivate, producing recurrent lesions. Typical clinical presentations include:
- Cold sores or fever blisters on or around the lips (commonly HSV-1).
- Genital herpes with sores on the external genitalia, perineum or inner thighs (commonly HSV-2 but also HSV-1).
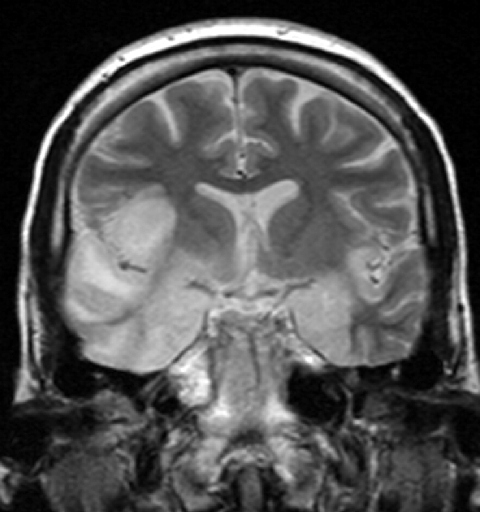
- Herpetic whitlow (painful finger infection), ocular herpes affecting the cornea, and less commonly encephalitis.
Reactivation can be triggered by stress, fever, ultraviolet light, immunosuppression or hormonal changes. Viral shedding can occur with or without visible lesions, which contributes to transmission.
Virus biology and types
HSV are enveloped, double-stranded DNA viruses. HSV-1 has a historical association with oral disease while HSV-2 more often involves the genital region, but either type can infect either site. The virus travels along peripheral nerves to sensory ganglia — the trigeminal ganglion for oral infection and the sacral ganglia for genital infection — where it persists in a latent state.
Diagnosis and treatment
Diagnosis is typically clinical when typical lesions are present. Laboratory tests include polymerase chain reaction (PCR) to detect viral DNA, viral culture from lesion swabs, and blood tests for antibodies to determine prior exposure. Antiviral medications such as acyclovir, valacyclovir and famciclovir reduce symptom severity, shorten outbreaks and can lower transmission risk when used as suppressive therapy, but they do not eradicate the latent virus. For more on testing and care see clinical resources.
Prevention and public health
Prevention centers on behavioral and medical strategies: avoiding direct contact with active lesions, using barrier protection like condoms which lower but do not eliminate transmission risk, antiviral suppressive therapy for people with frequent recurrences, and careful management during pregnancy to reduce neonatal exposure. Neonatal herpes is a serious but preventable complication when obstetric and infectious disease measures are applied. Public education and counselling help reduce stigma and support safer sexual and social practices. Additional information is available at public health guidance.
History, important distinctions and notable facts
The term "herpes" derives from a Greek root meaning "to creep," reflecting the appearance of spreading skin lesions. Modern virology established HSV as a distinct viral pathogen in the 20th century. Important distinctions include the difference between cold sores (herpes) and canker sores (aphthous ulcers), which are non-viral and occur inside the mouth. Serious but rare complications include herpes simplex encephalitis and vision loss from ocular involvement. Because asymptomatic viral shedding contributes to transmission, counseling about risk reduction remains central to management. For summaries and patient-focused material see educational links.
History
The genital manifestation of herpes simplex was already described by Hippocrates around 400 BC as a symptom of a spreading vesicular disease. The fact that the disease is also transmissible was known at the latest in Roman antiquity, as Emperor Tiberius forbade kissing during public ceremonies because the spread of vesicular disease was observed on the lips. This was documented by Aulus Cornelius Celsus as the first epidemic of a possible herpes disease. In 16th and 17th century Europe, herpes labialis was also widespread and its transmission through kissing was common knowledge. For example, William Shakespeare wrote in his well-known tragedy Romeo and Juliet, "O'er ladies' lips, who straight on kisses dream, Which oft the angry Mab with blisters plagues, because their breaths with sweetmeats are tainted." (Translation: "O'er ladies' lips that straight on kisses dream, Often the angry Mab with blisters plagues these, Because their breaths with sweetmeats are tainted"; erg. Explanation: The name Mab in the quotation refers to the fairy "Queen Mab", who appears in the work in a speech by Mercutio).
In 1736, Jean Astruc recognized genital herpes as a disease in its own right, and not as a variant of gonorrhea or syphilis as previously assumed. In 1883, the German dermatologist Paul Gerson Unna described the frequency of the disease and its co-occurrence with other venereal diseases. He also conducted the first histological studies on herpes simplex. After Wilhelm Gürtler was able to experimentally transfer the causative agent of herpes keratitis (herpes corneae) to a rabbit eye in 1913, Ernst Löwenstein found the identity of the causative agent of both diseases by transferring vesicular contents of herpes labialis to a rabbit eye. HSV was finally isolated and characterized for the first time from vesicle contents of a patient by Slavin and Gavett in 1946. The first electron microscopic imaging of herpes simplex viruses was achieved by Coriell in 1950, and it was not until the 1960s that Andre Nahmias and especially Karl Eduard Schneweis discovered that herpes simplex infections were caused by two different viral species, which researchers were able to distinguish on the basis of their different antigenicity.

Pathogen
Herpes simplex viruses
The two causative agents of herpes simplex infections - herpes simplex viruses 1 and 2 - which are also taxonomically and more correctly referred to as human herpes virus 1 and 2 (HHV-1/2), belong to the simplex virus genus of the family Herpesviridae. Members of this genus related to the herpes simplex viruses are also found in animals, where these viruses cause similar diseases in cattle, for example, or spider monkeys, macaques, and other guenon relatives. Although herpesviruses are generally strictly specialized to their respective hosts, rarely the macaque cercopithecine herpesvirus 1 (herpesvirus simiae), which is similar to HSV-1, can be transmitted to humans, where it can cause severe, generalized infections.
With a diameter of 140 to 180 nm, the herpes simplex viruses belong to the large viruses. A linear, double-stranded DNA is located in an icosahedral capsid as the genome. The capsid in turn is surrounded by a viral envelope, which leads to a sensitivity of the viruses to soaps, detergents or already mild disinfectants. Between the capsid and the viral envelope is a multitude of viral proteins, the so-called tegument proteins, which are responsible, among other things, for the regulation of gene expression in the host cell and the transition of the virus into a dormant latency stage. As a double-stranded DNA virus, the herpes simplex viruses are genetically stable; mutations and the emergence of natural variants are rather rare.
Transmission and dissemination
Herpes simplex viruses are distributed worldwide, and humans are their only natural reservoir. Since HSV-1 is already acquired through saliva contact and smear infection from infancy in normal family contact, it is common in the population. The virus shows an age-dependent seroprevalence, which reaches high percentages around the end of puberty and then increases only slightly further. In Germany, antibodies against HSV-1 could be detected in 84 to 92 % of the persons of an age-normalized random sample examination.
HSV-2 is transmitted through close mucosal contact when the virus is reactivated in the virus carrier and replicates again in epithelial cells. Viral shedding can also occur without visible lesions. The prevalence of antibodies against HSV-2 is distributed differently. It is particularly influenced by age and sexual activity; likewise, geographic distribution varies. In healthy blood donors or health surveillance, there have been frequencies ranging from 3% to 23% in the United States. This figure is significantly higher in patients who consulted a physician for another sexually transmitted disease (up to 55%) or engaged in commercial prostitution (up to 75%).
Infection mechanisms
In a primary infection, the HS viruses penetrate via the mucosal cells of the oral pharynx (predominantly HSV-1) and the genital tract (predominantly HSV-2). Areas at the transition from mucous membrane to normal skin are preferentially infected. Here the viruses multiply in the epithelial cells. The spread of the herpes simplex viruses within the epithelium occurs by destruction of the host cells and release of new virions or by fusion of adjacent cells, whereby the unenveloped virus capsids infect the new cell. Destruction of the epithelial cells manifests clinically in an inflammatory reaction, often forming an ulcer or inflammatory skin vesicle due to tissue destruction. The vesicular fluid is an exudate in which herpes simplex viruses accumulate in a high concentration (>100,000 PFU/µl).
By direct cell-cell contact or by virions in the interstitial fluid, HSV reaches the nerve endings of sensitive neurons, from which it is specifically taken up and transported along the microtubules and intermediate filaments of the axon to the cell body of the nerve. This retrograde axonal transport occurs by binding of the virus (as a naked viral capsid, possibly with residual tegument proteins and coat proteins) to kinesin-like proteins and dynein. The migration speed towards the cell body is about 0.7 µm per second.
Related articles
Author
AlegsaOnline.com Herpes simplex: causes, symptoms, transmission, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/43875