Esophageal cancer: types, causes, diagnosis, and management
Comprehensive overview of esophageal cancer: major types, symptoms, risk factors, diagnosis, staging, treatments, epidemiology and prevention strategies in accessible language.
Esophageal cancer is a malignancy that arises in the lining of the esophagus — the muscular tube that carries food from the throat to the stomach. It most commonly appears as two main histologic types: squamous cell carcinoma, which develops from the flat cells lining the upper and middle esophagus, and adenocarcinoma, which arises from glandular cells closer to the junction with the stomach. For an overview resource see esophageal cancer.
Image gallery
10 Images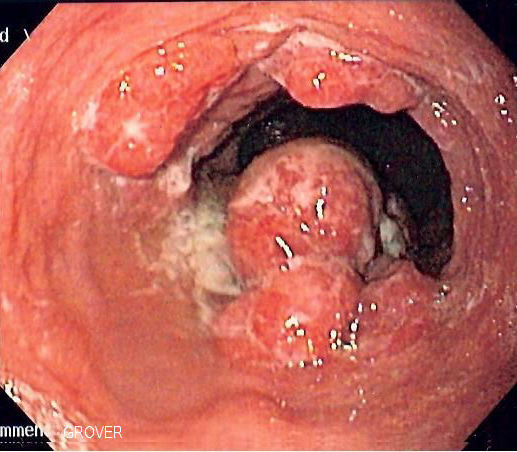








Typical signs and risk factors
Early disease may be asymptomatic; symptoms usually appear as the tumor grows. Common symptoms include progressive difficulty swallowing (dysphagia), unintentional weight loss, pain when swallowing (odynophagia), and persistent heartburn or chest discomfort. Risk factors differ by type but frequently include:
- For squamous cell carcinoma: tobacco use, heavy alcohol consumption, and certain dietary or environmental exposures.
- For adenocarcinoma: chronic gastroesophageal reflux disease (GERD), Barrett's esophagus, obesity, and smoking.
Diagnosis and staging
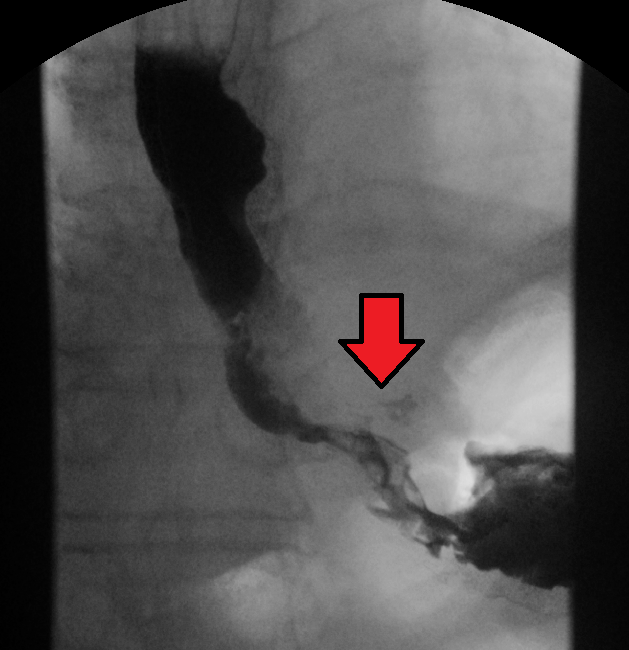
Diagnosis typically requires upper endoscopy with biopsy to confirm cancer type. Imaging tests such as CT, PET, and endoscopic ultrasound are used to determine the local extent of disease and to identify spread to lymph nodes or distant organs (staging). Accurate staging guides treatment planning and prognosis estimates.
Treatment approaches
Treatment depends on the stage, location, and patient fitness. Options commonly include surgery (esophagectomy) for localized disease, radiation therapy, systemic chemotherapy, and combinations of these modalities. In selected patients, chemoradiation may be used as primary therapy or to shrink tumors before surgery. Advances in targeted therapies and immunotherapy have expanded options for advanced disease, but outcomes vary and are often limited by late diagnosis.
Globally, the pattern of esophageal cancer varies: squamous cell carcinoma remains predominant in many parts of Asia and Africa, whereas adenocarcinoma has been increasing in incidence in Western countries over recent decades. Overall prognosis is guarded because many cases are diagnosed at an advanced stage, highlighting the importance of awareness and early evaluation of persistent swallowing problems or unexplained weight loss.
Prevention strategies focus on reducing modifiable risks: smoking cessation, limiting alcohol, managing reflux and obesity, and surveillance of high-risk conditions such as Barrett's esophagus. Regular medical follow-up and timely investigation of symptoms can improve the chances of earlier detection and more effective treatment.
Questions and answers
Q: What is esophageal cancer?
A: Esophageal cancer is a type of cancer that occurs in the esophagus.
Q: What are the most common types of esophageal cancer?
A: The most common types of esophageal cancer are squamous cell cancer and adenocarcinoma.
Q: What percentage of all esophageal cancer is squamous cell cancer?
A: About 90-95% of all esophageal cancer worldwide is squamous cell cancer.
Q: What percentage of esophageal cancer in the United States is adenocarcinoma?
A: About 50-80% of all esophageal cancer in the United States is adenocarcinoma.
Q: Where does squamous cell cancer start?
A: Squamous cell cancer starts from the cells that line the upper part of the esophagus.
Q: Where does adenocarcinoma start?
A: Adenocarcinoma starts from glandular cells that are present at the lining of the esophagus and stomach.
Q: How many types of esophageal cancer are there?
A: There are many types of esophageal cancer, but the most common types are squamous cell cancer and adenocarcinoma.
Related articles
Author
AlegsaOnline.com Esophageal cancer: types, causes, diagnosis, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/32188
Sources
- mountsinai.org : Esophageal cancer