Epstein–Barr virus (EBV): overview, biology, clinical impact and public health
Epstein–Barr virus (EBV) is a common human herpesvirus that causes infectious mononucleosis, establishes lifelong latency in B cells, and is linked to several cancers and immune disorders.
Overview
The Epstein–Barr virus (EBV), also known as human herpesvirus 4, is a widespread DNA virus in the herpesvirus family. Most people worldwide are infected at some point in life and retain the virus in a latent form. Primary infection in childhood is often asymptomatic, while infection during adolescence or young adulthood commonly produces infectious mononucleosis (also called glandular fever). EBV can be transmitted by close contact involving saliva and other body fluids; these routes are described in more detail below.
Image gallery
4 Images


Virology and life cycle
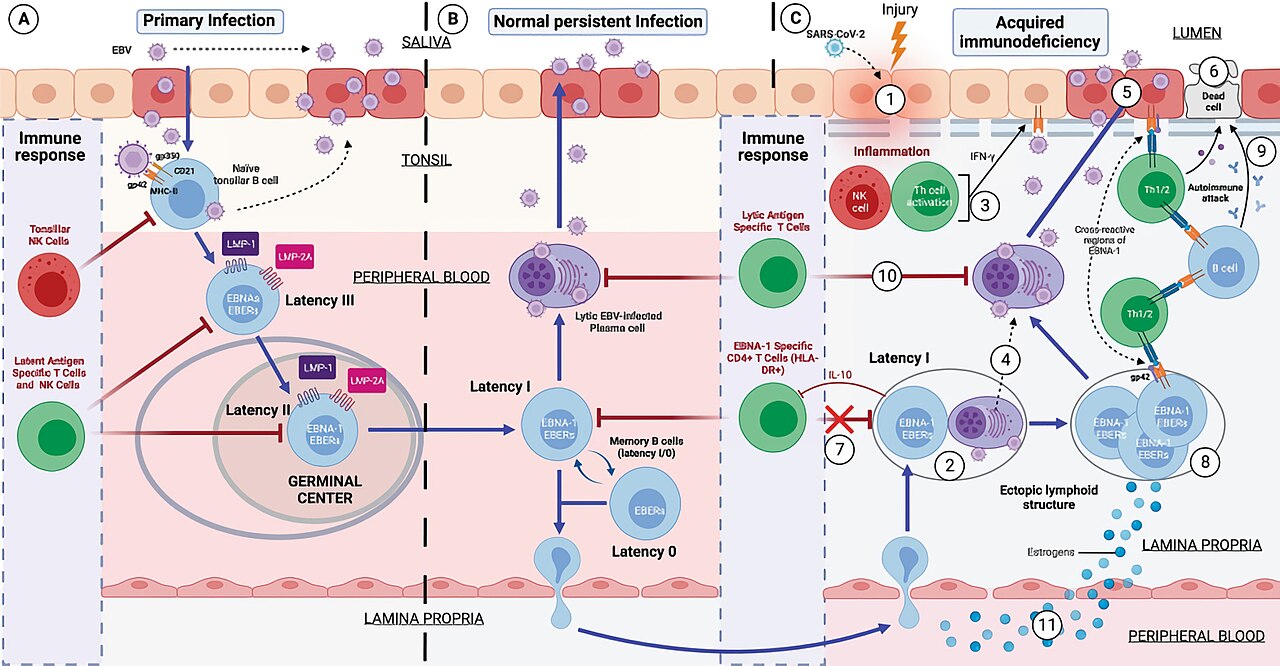
EBV infects two main cell types: B lymphocytes of the adaptive immune system and mucosal epithelial cells. The virus attaches to cell surface receptors and enters cells, then either begins replicating (lytic cycle) or establishes a nonproductive, long-term infection known as latency. Latent EBV persists in B cells for the person's lifetime and can periodically reactivate. Different patterns of gene expression during latency are linked with distinct biological behaviours and with some EBV-related malignancies. For a concise placement of EBV among related viruses, see the herpes family summary here.
Clinical features, diagnosis and management
When symptomatic, EBV infection most often causes infectious mononucleosis. Typical features include fever, sore throat, swollen lymph nodes, and fatigue; the spleen may be enlarged. Complications are uncommon but can include splenic rupture, airway compromise from severe tonsillar swelling, or prolonged fatigue. In people with weakened immunity, EBV can cause more severe or chronic disease.
- Common clinical signs: fever, pharyngitis, lymphadenopathy, fatigue.
- Diagnostic approaches: heterophile antibody tests (Monospot) and EBV-specific serology (viral capsid antigen and nuclear antigen antibodies) and, where needed, molecular tests for viral DNA.
- Treatment: largely supportive (rest, fluids, analgesics); no broadly approved vaccine or curative antiviral is in routine clinical use yet.
Transmission, epidemiology and prevention
EBV spreads mainly through saliva, which explains why close personal contact and sharing of utensils or drinks can transmit the virus. Studies also document virus in genital secretions and blood, though saliva is the dominant route. In many parts of the world, most children are infected and develop immunity early; in more developed settings, primary infection is often delayed until adolescence when symptomatic illness is more likely. Practical preventive measures focus on reducing saliva-sharing behaviours; vaccine development remains an active area of research.
Associations with cancer and immune disorders
EBV is linked to several malignancies and immune-mediated conditions. It is implicated in some cases of Hodgkin lymphoma, Burkitt lymphoma, nasopharyngeal carcinoma and a subset of gastric carcinomas; the strength of association varies by cancer type and geography. EBV infection has also been associated with a higher risk of certain autoimmune diseases in epidemiological studies. Because the virus can drive B-cell proliferation and alter immune signalling, it is of particular concern in people with impaired immune control, including individuals living with HIV.
Notable facts and research directions
Key points include: EBV establishes lifelong latency after primary infection; it can reactivate intermittently; and it contributes to a measurable burden of disease beyond mononucleosis, especially in oncology and immunology. Current research priorities include better understanding of latency mechanisms, development of vaccines and targeted antiviral or immunotherapeutic strategies, and clarifying causal pathways linking EBV to autoimmune and malignant diseases. For summaries of EBV's links to cancer and immune conditions see resources on associated cancers and autoimmune diseases. Transmission guidance is available related to saliva and bodily fluids: saliva and genital exposure risks. Clinical terminology and patient information often use terms like glandular fever and discuss effects on the immune system.
Because EBV intersects virology, oncology and immunology, it remains a subject of active study and clinical concern. Continued surveillance, supportive clinical care for symptomatic cases, and progress toward preventive vaccines are important public-health goals.
Questions and answers
Q: What is the Epstein-Barr virus?
A: The Epstein-Barr virus (EBV) is a type of herpesvirus that is one of eight viruses in the herpes family. It is one of the most common viruses in humans and is best known as the cause of infectious mononucleosis (glandular fever).
Q: How does EBV spread?
A: EBV spreads through oral transfer, which means it can be transferred by saliva or genital secretions.
Q: How many people are infected with EBV?
A: In the United States, about half of all five-year-old children and about 90 percent of adults have evidence of previous infection. Many children become infected with EBV but usually experience no symptoms or just mild, brief illnesses.
Q: What happens when someone becomes infected with EBV during adolescence?
A: When someone becomes infected with EBV during adolescence, it causes glandular fever 35 to 50 percent of the time.
Q: Where does EBV infect in the body?
A: EBV infects B cells in the immune system and epithelial cells.
Q: Does non-active EBV stay in a person's body for life after an initial infection has been brought under control?
A: Yes, once an initial infection has been brought under control, non-active EBV stays in a person's B cells for life.
Q: How many cancer cases per year may be caused by or associated with EBV? A: Approximately 200,000 cancer cases per year may be caused by or associated with EBV.
Related articles
Author
AlegsaOnline.com Epstein–Barr virus (EBV): overview, biology, clinical impact and public health Leandro Alegsa
URL: https://en.alegsaonline.com/art/31797
Sources
- doi.org : 10.1007/s11604-008-0291-2
- pubmed.ncbi.nlm.nih.gov : 19373526
- ncbi.nlm.nih.gov : "Oral manifestations in the era of HAART"
- pubmed.ncbi.nlm.nih.gov : 12656429
- doi.org : 10.1016/j.berh.2008.09.007
- pubmed.ncbi.nlm.nih.gov : 19028369
- doi.org : 10.1016/j.autrev.2011.08.005
- pubmed.ncbi.nlm.nih.gov : 21871974
- ncbi.nlm.nih.gov : "CD8+ T-cell deficiency, Epstein–Barr virus infection, Vitamin D deficiency, and steps to autoimmunity: a unifying hypothesis"
- doi.org : 10.1155/2012/189096
- pubmed.ncbi.nlm.nih.gov : 22312480
- doi.org : 10.1007/s11481-010-9201-3
- pubmed.ncbi.nlm.nih.gov : 20369303