Ectopic pregnancy: causes, diagnosis, treatment and risks
Ectopic pregnancy occurs when a fertilized egg implants outside the uterine cavity. This article explains locations, symptoms, diagnosis, treatment options, risks and important distinctions.
Overview
An ectopic pregnancy happens when a fertilized egg implants and begins to develop somewhere other than the inside of the uterine cavity. In a normal pregnancy the embryo attaches to the implantation site on the uterine wall and continues growth into a fetus. An embryo that implants outside the uterus cannot develop into a viable pregnancy and may endanger the pregnant person if not identified and treated.
Image gallery
10 Images







Common locations and terminology
Most ectopic pregnancies occur in a fallopian tube, which is why the term "tubal pregnancy" is frequently used. Other, less common locations include the surface of an ovary, the lining of the cervix, the abdominal cavity, and scars from previous cesarean sections. The uterus itself (uterine cavity) is the only location compatible with a normal live birth; implants elsewhere are considered ectopic.
Causes and risk factors
An ectopic implantation usually reflects some interference with the transport of the fertilized egg from the ovary toward the uterine cavity. Known factors associated with an increased risk include prior tubal surgery, pelvic inflammatory disease, previous ectopic pregnancy, certain assisted reproductive procedures, and conditions that alter tubal anatomy or function. Lifestyle factors such as smoking and older maternal age are also associated with higher risk. The ovaries (ovaries) and fallopian tubes are frequently involved in the underlying processes that allow ectopic implantation.
Signs, diagnosis and evaluation
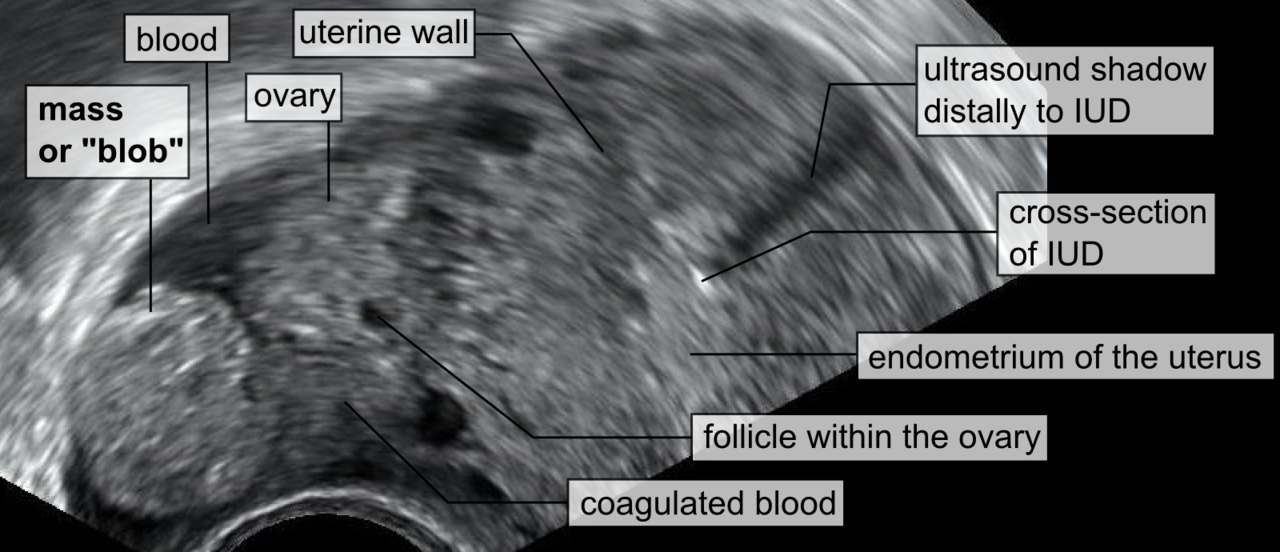
Symptoms commonly include unilateral abdominal pain, vaginal bleeding, and shoulder tip pain from diaphragmatic irritation when internal bleeding is present. Some people may have only mild or nonspecific symptoms. Diagnosis is based on a combination of clinical examination, serial measurement of pregnancy hormone levels (hCG), and imaging—most often transvaginal ultrasound. When imaging is inconclusive, careful follow-up and repeat testing are needed because an early normal intrauterine pregnancy can appear similar to an ectopic one at first.
Treatment and management
Treatment choices depend on the location, size, symptoms and stability of the patient. Options include:
- Expectant management with close monitoring when the ectopic is small and resolving on its own.
- Medical treatment, typically with a single-dose or multi-dose regimen of a medication that stops rapidly dividing cells, in carefully selected cases.
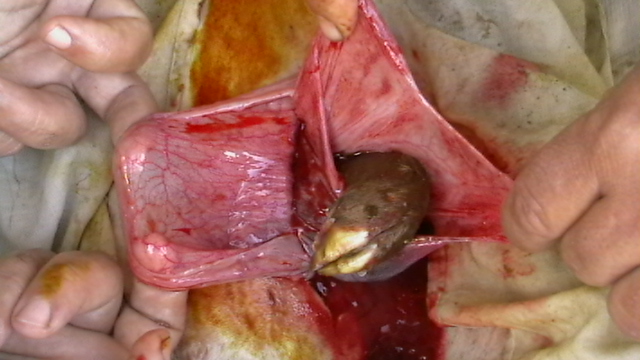
- Surgical management—most often minimally invasive laparoscopy—to remove the ectopic tissue and, if necessary, repair or remove the affected tube or structure. Emergency surgery is required if rupture and significant internal bleeding occur.
Prognosis, future fertility and prevention
An ectopic pregnancy is not viable and cannot result in a live birth. With timely diagnosis and appropriate care, most people recover and maintain fertility, though future tubal function can be affected depending on the extent of damage and the treatment performed. Measures that reduce pelvic infection risk and early medical evaluation of suspicious symptoms can lower likelihood or consequences of ectopic implantation.
Notable facts and distinctions
Some ectopic implantations are extremely rare, such as those within a previous cesarean scar or implanted on abdominal organs, and they present additional clinical challenges. Clinical pathways emphasize early ultrasound and hormone testing to distinguish an ectopic pregnancy from a very early intrauterine pregnancy or other causes of pelvic pain and bleeding. For reliable patient information and clinical guidance, see reputable medical sources and specialist consultation—resources are often available through patient education pages and professional protocols (fetal development and pregnancy resources, cervical pregnancy information)."
When discussing diagnosis and treatment options, clinicians tailor decisions to the individual patient, balancing safety, future fertility goals, and the urgency of the clinical situation.
Questions and answers
Q: What is an ectopic pregnancy?
A: An ectopic pregnancy is when an embryo implants itself (sticks to somewhere) outside the uterus.
Q: Where does the embryo usually implant itself in a normal pregnancy?
A: In a normal pregnancy, the embryo implants (sticks) itself into the wall of the uterus.
Q: Why are most ectopic pregnancies called tubal pregnancies?
A: Most ectopic pregnancies happen in a Fallopian tube, which is one of the two tubes that connect the ovaries and the uterus.
Q: Can ectopic pregnancies become normal pregnancies and result in a baby?
A: No, ectopic pregnancies cannot become normal pregnancies and will not result in a baby.
Q: What health problems can ectopic pregnancies cause for the mother?
A: Ectopic pregnancies can cause serious health problems for the mother.
Q: Where else can ectopic pregnancies happen aside from the Fallopian tube?
A: Rarely, ectopic pregnancies can happen in an ovary or in the cervix.
Q: What is the uterus and why is it important in pregnancy?
A: The uterus is the only place in the body where an embryo can grow into a fetus. It is important in pregnancy because it provides an environment for the developing embryo and helps nourish and protect it.
Related articles
Author
AlegsaOnline.com Ectopic pregnancy: causes, diagnosis, treatment and risks Leandro Alegsa
URL: https://en.alegsaonline.com/art/29989
Sources
- ncbi.nlm.nih.gov : Ectopic Pregnancy.
- mayoclinic.com : Ectopic Pregnancy: Risk Factors.
- mayoclinic.com : Ectopic Pregnancy: Symptoms.
- webmd.com : Ectopic (Tubal) Pregnancy Causes, Symptoms, Diagnosis, Treatment and Prevention.
- webmd.com : Fertility After Ectopic Pregnancy.