Diffuse axonal injury
Diffuse axonal injury (DAI) is brain damage caused by shearing forces that disrupt axons across wide areas, often producing coma and long-term disability; diagnosis and treatment focus on supportive care and rehabilitation.
Overview
Diffuse axonal injury (DAI) is a form of traumatic brain injury in which widespread damage to axons — the long, cable-like processes of neurons — occurs across multiple regions of the brain rather than at a single focal point. It is a common cause of unconsciousness and long-term neurological impairment following head trauma. DAI primarily affects the brain's white matter, the bundles of nerve fibers that connect different brain regions, and is often associated with prolonged coma and persistent disorders of consciousness such as the vegetative state.
Image gallery
3 Images

Mechanism and pathology
The injury typically results from high-velocity acceleration, deceleration, or rotational forces that produce shearing stress between brain tissues of different densities. These mechanical forces stretch, twist, or tear axons microscopically. Pathological findings include axonal swelling, disconnection, and the formation of retraction bulbs; these changes can be widely distributed but are characteristically concentrated at the gray–white matter junction, in the corpus callosum, and in the brainstem. Even when gross imaging appears normal, microscopic axonal injury can underlie significant clinical deficits.
Clinical features and severity
Symptoms vary with severity. Severe DAI often causes immediate loss of consciousness and prolonged coma. Milder forms may produce transient confusion, headache, or cognitive and emotional difficulties. Because DAI affects connections rather than isolated cortical areas, common deficits include impaired attention, slowed processing speed, memory problems, and changes in arousal or behavior. Some authors consider concussion to be on the mild end of the spectrum of diffuse axonal injury; in a clinical context, brief loss of consciousness or post-traumatic amnesia may reflect mild axonal trauma (concussion).
Diagnosis
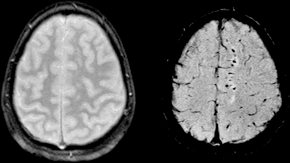
Diagnosing DAI relies on clinical assessment and neuroimaging. Standard CT scans may miss microscopic axonal damage, so MRI techniques — including diffusion-weighted imaging, susceptibility-weighted imaging, and FLAIR sequences — are more sensitive to the small hemorrhagic and non-hemorrhagic lesions typical of DAI. Neurological examination, duration of coma, and electroencephalography can help gauge severity and prognosis. Where available, specialized MRI sequences are often used to better visualize white matter disruption.
Treatment and prognosis
There is no specific therapy to repair axons once damaged; acute management focuses on protecting the brain from secondary injury by stabilizing airway, breathing and circulation, controlling intracranial pressure, and treating complications such as seizures. Rehabilitation — including physical, occupational, speech, and cognitive therapies — is central to recovery and long-term functional improvement. Prognosis depends on injury severity, extent of brainstem involvement, and the patient's age and overall health; while some patients regain significant function, many experience persistent disability or prolonged disorders of consciousness. Severe DAI is a frequent contributor to prolonged coma after head trauma (coma) and occurs in a high proportion of major head injuries.
Causes, epidemiology, and notable distinctions
DAI commonly arises from motor vehicle collisions, falls, sports injuries, and assaults — situations that generate rapid head movement rather than a single focal impact. It is one of the most frequent pathological mechanisms in severe traumatic brain injury and can accompany other focal lesions. Distinguishing DAI from focal contusions or hematomas is important for prognosis and management: whereas focal injuries are localized and often amenable to surgical intervention, DAI is a diffuse, primarily microscopic process treated mainly with medical and rehabilitative strategies. For broader context on traumatic brain injury, see traumatic brain injury resources.
- Commonly affected structures: corpus callosum, brainstem, and subcortical white matter.
- Imaging: MRI (diffusion and susceptibility sequences) is more sensitive than CT.
- Outcome: ranges from full recovery in mild cases to severe, persistent impairment in extensive injuries.
For more detailed clinical guidance and recent advances in imaging or rehabilitation approaches, consult specialized neurological and trauma references or institutional protocols (TBI overview, white matter studies, disorders of consciousness, coma assessment, concussion resources).
Questions and answers
Q: What is diffuse axonal injury?
A: Diffuse axonal injury is a common form of traumatic brain injury where the damage occurs over a larger area of the brain.
Q: Which part of the brain is mainly affected by diffuse axonal injury?
A: Diffuse axonal injury mainly damages the white matter of the brain.
Q: How does diffuse axonal injury differ from other types of traumatic brain injury?
A: In other types of traumatic brain injury, the damage is focused on one area of the brain, but in diffuse axonal injury, the damage occurs over a larger area of the brain.
Q: What is the incidence of diffuse axonal injury in cases of severe head trauma?
A: Diffuse axonal injury occurs in about half of all cases of severe head trauma.
Q: What is the impact of diffuse axonal injury on patients?
A: Diffuse axonal injury is one of the major causes of unconsciousness and persistent vegetative state after head trauma. Over 90 percent of patients with severe DAI never regain consciousness, and those who do wake up often remain significantly impaired.
Q: Can diffuse axonal injury occur in milder forms?
A: Yes, other authors state that diffuse axonal injury can occur in every degree of severity from (very) mild or moderate to (very) severe.
Q: How is concussion related to diffuse axonal injury?
A: Concussion may be a milder type of diffuse axonal injury.
Related articles
Author
AlegsaOnline.com Diffuse axonal injury Leandro Alegsa
URL: https://en.alegsaonline.com/art/27355
Sources
- emedicine.com : Diffuse axonal injury
- emedicine.com : Penetrating head trauma
- nro.sagepub.com : Axonal damage in traumatic brain injury
- nts.prolekare.cz : "An outline of the current concepts of mild brain injury with emphasis on the adult population"