Diastole: the heart's relaxation and filling phase — physiology and clinical importance
Diastole is the phase of the cardiac cycle when the heart relaxes and fills with blood. This article explains its phases, relation to blood pressure, clinical significance and how diastolic dysfunction is assessed.
Overview
Diastole is the portion of the cardiac cycle during which the heart muscle relaxes after contraction and the chambers refill with blood. It contrasts with systole, when the heart contracts to eject blood. Proper diastolic function is essential for adequate cardiac output because filling during relaxation determines the volume available for the next beat. In everyday language, diastolic pressure is often referred to as the lower number in a blood pressure reading, reflecting arterial pressure while the heart is relaxed.
Image gallery
1 Image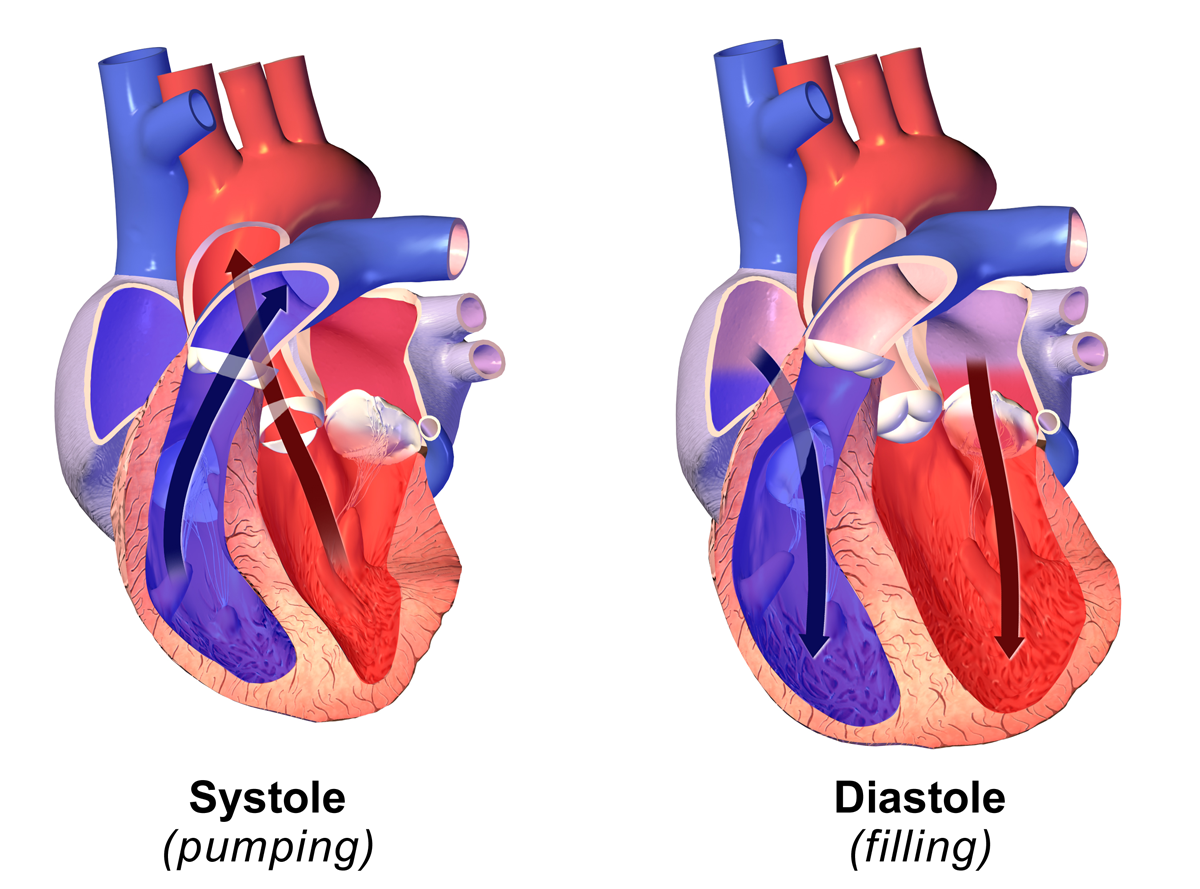
Phases and mechanics
Diastole is not a single moment but a sequence of events that coordinate the left and right sides of the heart. The main subphases commonly described are:
- Isovolumetric relaxation — valves close and the ventricles relax without changing volume.
- Rapid ventricular filling — blood flows from the atria into the ventricles when the atrioventricular valves open.
- Diastasis — a slower filling phase as pressures equilibrate.
- Atrial contraction (atrial systole) — a final push from the atria tops up ventricular volume just before the next systole.
Relation to blood pressure and heart rate
Diastolic arterial pressure is the pressure in the large arteries when the heart is relaxed and is measured in millimetres of mercury (mmHg) in clinical practice. The length of diastole varies with heart rate: when heart rate increases, diastole shortens proportionally more than systole. Because filling time falls at higher rates, very rapid heartbeats can reduce ventricular filling and cardiac output if diastolic time becomes too brief.
Clinical importance and common disorders
Abnormal diastolic function can cause symptoms of breathlessness and fatigue even when systolic contraction (the pumping ability) appears normal. Conditions associated with impaired diastole include increased stiffness of the ventricle due to aging or hypertrophy, high blood pressure, ischemic heart disease, and restrictive cardiomyopathies. Clinicians may refer to "diastolic dysfunction" or to heart failure with preserved ejection fraction (HFpEF) when relaxation or filling is inadequate despite a preserved ejection fraction.
Measurement and assessment
Diastolic performance is assessed in several ways. Blood pressure measurement provides the arterial diastolic value. Echocardiography offers detailed assessment of ventricular filling patterns, chamber sizes, valve function and estimates of filling pressures. Electrocardiography and invasive catheter studies can give additional timing and pressure information when needed. Interpreting these tests requires integrating symptoms, imaging, and risk factors such as hypertension and coronary disease.
History, terminology and notable facts
The word "diastole" comes from the Greek term for stretching or opening. The concept of diastole as a distinct part of the heartbeat developed over centuries as instruments and physiological understanding improved. Notable practical points:
- In blood pressure readings the diastolic value is the lower number and indicates arterial pressure during relaxation.
- Diastolic murmurs and extra sounds can signal specific valve or filling abnormalities.
- Age and chronic high blood pressure commonly alter diastolic properties of the heart and vessels.
Questions and answers
Q: What is diastole?
A: Diastole is the period of time during a heartbeat where the heart fills with blood after a contraction.
Q: What is systole?
A: Systole is the period of time during a heartbeat where the heart contracts and pushes blood through the body.
Q: What is the origin of the word diastole?
A: The word diastole comes from the Greek word διαστολη, which means expanding or opening.
Q: How does the heart function during diastole?
A: During diastole, the heart relaxes and expands to allow blood to flow into the chambers.
Q: Why is diastole considered the opposite of systole?
A: Systole and diastole are considered opposites because systole is the period of contraction where the heart pumps blood out, while diastole is the period of relaxation where blood fills the heart.
Q: How is diastole important for overall heart health?
A: Diastole is important because it allows the heart to refill with blood, which is necessary to maintain healthy blood flow and oxygenation throughout the body.
Q: What does it mean when someone has diastolic dysfunction?
A: Diastolic dysfunction is a condition where the heart has difficulty filling with blood during diastole, which can lead to problems with blood flow and potential heart failure.
Related articles
Author
AlegsaOnline.com Diastole: the heart's relaxation and filling phase — physiology and clinical importance Leandro Alegsa
URL: https://en.alegsaonline.com/art/27152
Sources
- merriam-webster.com : Diastole
- bioline.org.br : bioline.org.br/request?mj04008