Diabetes mellitus
A chronic metabolic disorder caused by impaired insulin action or secretion, leading to high blood glucose and long-term health risks; includes types, causes, diagnosis, treatment, and prevention.
Overview
Diabetes mellitus is a group of metabolic disorders characterized by elevated blood glucose (hyperglycemia) resulting from defects in insulin secretion, insulin action, or both. The condition is distinct from diabetes insipidus, which affects water balance and is unrelated to blood sugar regulation. In everyday language, “diabetes” usually refers to diabetes mellitus; people who live with the condition are often called diabetics.
Image gallery
10 Images






Glucose, hormones and normal regulation
Glucose is a simple sugar and a primary cellular fuel; it is one kind of carbohydrate the body uses for energy. Common table sugar (sucrose) is chemically different from glucose and is handled differently by digestion and metabolism; see sucrose for that distinction. Foods and drinks can contain high amounts of glucose or glucose-yielding carbohydrates, for example some soft drinks and certain fruits, and can raise blood sugar rapidly when consumed in quantity. The body normally keeps blood glucose within a narrow range through a coordinated hormonal response; when that system fails, diabetes can develop.
How insulin and the pancreas work
The hormone insulin, produced by the pancreas, is central to lowering blood glucose after meals by signaling cells throughout the body to absorb and use glucose. Excess glucose is stored as glycogen in liver and muscle. Diabetes mellitus arises either when the pancreas does not produce enough insulin, when tissues fail to respond properly to insulin (insulin resistance), or both. The term hormones is often used when discussing the chemical signals that regulate these processes.
Types and common features
Clinically, diabetes is grouped into several types with different causes and patterns:
- Type 1 diabetes: usually immune-mediated destruction of insulin-producing cells, requiring insulin replacement.
- Type 2 diabetes: characterized by insulin resistance and relative insulin insufficiency; the most common form in adults.
- Gestational diabetes: glucose intolerance first identified during pregnancy, which increases risk for later diabetes.
Typical symptoms include excessive thirst, frequent urination, unexplained weight loss, fatigue, and blurred vision. Symptoms may appear abruptly in type 1 but more gradually in type 2.
Diagnosis, monitoring and complications
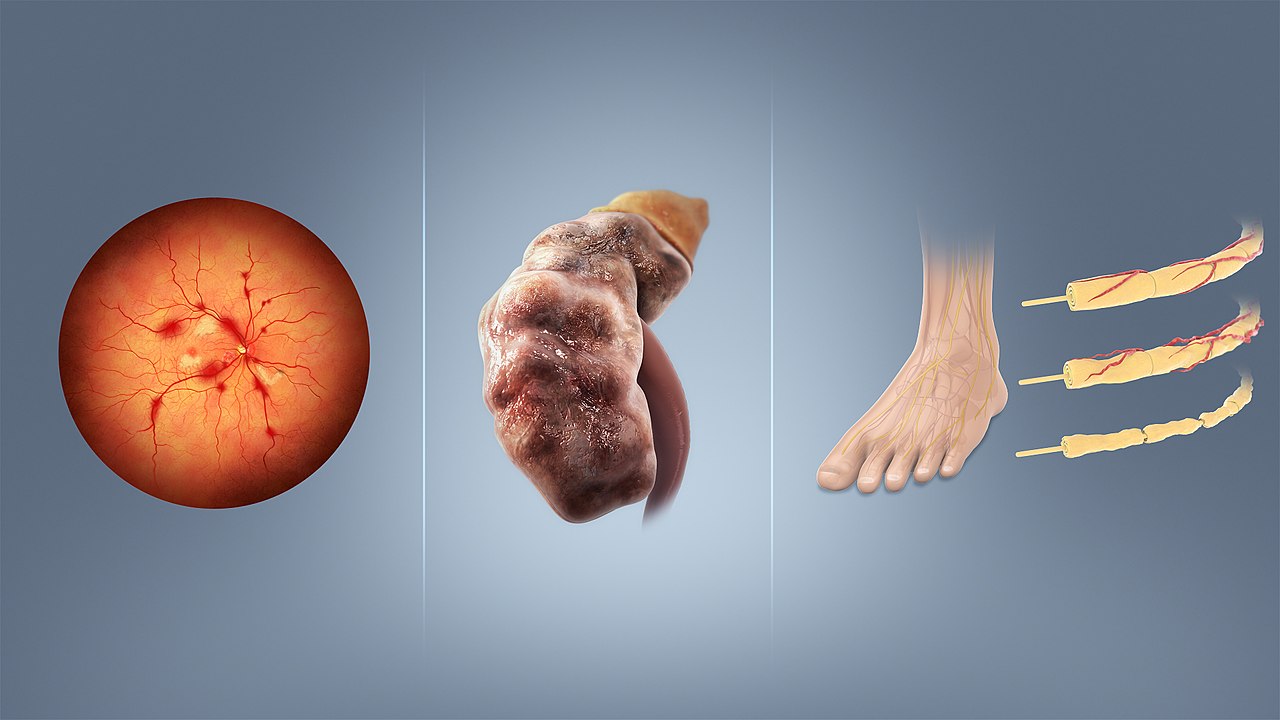
Diagnosis relies on measuring blood glucose with established tests such as fasting glucose, oral glucose tolerance, and long-term average measurements like glycated hemoglobin. People with diabetes monitor glucose levels to guide therapy and reduce risk. Chronic high blood glucose damages small blood vessels (microvascular complications such as eye, kidney, and nerve disease) and larger vessels (macrovascular disease leading to heart attack and stroke). Prompt detection and consistent management reduce these risks.
Treatment, prevention and historical notes
Treatment strategies combine lifestyle measures—healthy diet, physical activity, and weight management—with medicines that improve insulin sensitivity or provide insulin directly. Oral drugs and injectable therapies are selected based on type of diabetes, severity, and individual factors. Preventive approaches target modifiable risks such as excess weight and inactivity, and public health efforts aim to improve screening and education. The understanding and treatment of diabetes advanced significantly after the discovery of insulin therapy in the early 1920s, and research continues on technologies like continuous glucose monitoring and closed-loop "artificial pancreas" systems to improve outcomes.
Important distinctions and further reading
Remember that diabetes mellitus is a metabolic disorder primarily involving glucose regulation and insulin, while diabetes insipidus involves antidiuretic hormone pathways and water balance. For concise introductions to specific topics mentioned above, see entries on insulin, the pancreas, carbohydrates, and how hormones control metabolism. Typical sources for lay readers and patients include clinical guidelines and patient education pages that explain testing, lifestyle advice, and medication options. Additional technical or historical material can be found through specialist reviews and textbooks; for a practical short guide, consult links on diet and food sources of sugar, such as soft drinks, fruits, and information about foods with high concentrations of sugars.
For metabolic background on energy use and storage see discussions of energy metabolism, cellular cells, and storage molecules such as glycogen. Each of these topics sheds light on how dysregulation leads to the symptoms and complications associated with diabetes mellitus.
Physiological basics
The digestive system breaks down the carbohydrates ingested with food (from fruits, cereal products, potatoes, corn, rice) into glucose (dextrose), which is then absorbed through the intestinal wall into the blood and distributed throughout the body.
The pancreas produces the hormone insulin in the β-cells of the islets of Langerhans. As a messenger substance, insulin causes the transport of glucose into the cell interior, where the glucose is subsequently consumed for energy production (glycolysis). In addition, insulin also causes glucose to be stored in the form of glycogen in the liver as well as in the muscle cells, which keeps the blood glucose level constant within narrow limits (approx. 80-120 mg/dl or 4.5-6.7 mmol/l) after food intake.
Even during long periods of fasting, the blood sugar level remains at a normal level, which in turn is mainly ensured by the liver, on the one hand by the previously formed glycogen being split back into glucose and released back into the blood, and on the other hand by the liver constantly producing new glucose biochemically (gluconeogenesis).
If the insulin-producing β-cells no longer produce enough insulin or no insulin at all, or are no longer present at all, e.g. due to inflammation or surgery, both glucose uptake into the body's cells and the inhibition of new glucose formation in the liver (which can produce up to 500 grams of new glucose per day in humans) are therefore missing. This new formation explains the rise in blood glucose levels in diabetics, e.g. in the early morning when they are fasting (see also Dawn phenomenon).
In diabetes mellitus, the ingested glucose remains in the blood, or the body's own new glucose formation in the liver continues unchecked and constantly supplies glucose, which balances or even exceeds the continuous consumption and as a result causes the blood sugar to rise. It is a very complex and dynamic biochemical process in which inflows, outflows, new formation and degradation of glucose must be constantly balanced, i.e. accounted for. In order to understand these interrelationships - and thus the disease and how to deal with it - affected patients must be carefully informed and advised and, if necessary, trained, for example in the preparation of suitable dietary plans.
In addition, insulin has another, third effect. It is the only hormone in the human body that builds up body fat and also ensures that this fat remains in the depots (so-called adipogenic effect).
A major characteristic of severe, persistent insulin deficiency is therefore also extreme weight loss due to the elimination of the adipogenic effect, in particular the breakdown of body fat and (muscle) protein for energy production.

Classification of diabetes mellitus into types
In 1965, the World Health Organization (WHO) published a distinction between different types of diabetes in its "Recommendations on Classification and Diagnosis".
In 1997, the American Diabetes Association (ADA) changed the criteria for classification and diagnosis, which were adopted by the WHO in 1998 and by the German Diabetes Association (DDG) in 2000. In the model, a distinction was no longer made between insulin-dependent diabetes mellitus (IDDM) and non-insulin-dependent diabetes mellitus (NIDDM), as this classification only refers to treatment and not to the cause of the disease. Since 2009, the definition no longer distinguishes between subgroups a and b. The ranking of diabetes types from A-H was also abandoned.
Classification until 1997
Until that date, diabetes mellitus was divided into four groups according to the type of treatment, the fifth designated that the disease is not present:
- NIR: (non-insulin-requiring) treatment without external insulin supply, e.g. with diet and/or oral antidiabetics only.
- IRC: (insulin requiring for control) In addition to the body's own insulin, external insulin is also required to lower elevated blood glucose levels.
- IRS: (insulin requiring for survival) External insulin supply is required for survival. According to the new classification, these are type 1 diabetes and type 2 diabetes with severely reduced or discontinued own insulin production.
- IGT: (impaired glucose tolerance) Impaired glucose tolerance.
- ND: (non diabetic) Not suffering from diabetes.
Diabetes types since 1998
Since that date, all organizations divided the disease into the following four types according to the cause:
- Diabetes mellitus type 1: T-cell mediated autoimmune disease with destruction especially of the beta cells of the islets of Langerhans in the pancreas, usually leading to absolute insulin deficiency.
- Diabetes mellitus type 2: Different combinations of insulin resistance, hyperinsulinism, relative insulin deficiency, secretion disorders
- Type 2a: without obesity (adiposity)
- Type 2b: with obesity
- Other specific types of diabetes
- A: genetic defects of the beta cells of the islets of Langerhans (impaired insulin secretion)
- B: rare genetic defects of insulin action
- C: Pancreas diseased or destroyed
- D: Diabetes due to hormonal disorders (endocrinopathies)
- E: Diabetes caused by medications or chemicals (drugs, toxins).
- F: Diabetes mellitus due to infections
- G: unusual forms of immune-mediated diabetes
- H: other genetic syndromes associated with diabetes
- Gestational diabetes (pregnancy diabetes)
Diabetes types according to the DDG 2009 guidelines
Based on the report of the WHO Commission of 1999, the following criteria are used for classification according to the guidelines of the DDG 2009:
- Type 1 diabetes mellitus: Destruction of the beta cells of the pancreatic islets of Langerhans leads to absolute insulin deficiency.
- Type 2 diabetes mellitus: Can range from (genetic) insulin resistance with relative insulin deficiency to absolute insulin deficiency later in the course of the disease. It is often associated with other metabolic syndrome problems.
- Other specific types of diabetes
- Diseases of the exocrine pancreas (e.g. pancreatitis, cystic fibrosis, haemochromatosis)
- Endocrinopathies (e.g. Cushing's syndrome, acromegaly, pheochromocytoma)
- Drug-chemically induced (e.g. glucocorticoids, neuroleptics, alpha-interferon, pentamidine)
- Genetic defects of β-cell function (e.g. MODY forms)
- Genetic defects of insulin action
- Other genetic syndromes that may be associated with diabetes
- Rare forms of autoimmune-mediated diabetes.
- Gestational diabetes: glucose tolerance disorder first encountered or diagnosed during pregnancy. This includes:
· Initial manifestation of type 1 diabetes
· Initial manifestation of type 2 diabetes
· Initial manifestation of other specific types of diabetes
· Preconceptionally manifest but undiagnosed diabetes mellitus (type 2), especially to be assumed in the case of glucose tolerance disorders already in the 1st trimester.
This classification was confirmed by the DDG in 2011 as part of an update of the guidelines.
Other terms
- Juvenile diabetes mellitus or "juvenile diabetes mellitus" is the outdated term for type 1 diabetes.
- Adult-onset diabetes mellitus or "adult-onset diabetes" used to be the name given to type 2 diabetes. Both terms are still widely used, but do not reflect the current state of science and are therefore no longer included in the current classifications.
- LADA: Type 1 diabetes mellitus also includes LADA (latent autoimmune diabetes with onset in adults). This form concerns the autoimmune diabetes that develops in older adults, which after a relatively short time no longer responds to oral medication and becomes insulin-dependent. Typical is the detection of the GAD (=glutamate decarboxylase) antibody.
- MODY: MODY (maturity onset diabetes of the young) corresponds to the progression form of type 2 diabetes, but without the occurrence of obesity and insulin resistance, instead it already occurs in children and adolescents.
- IDDM: Abbreviation for insulin dependent diabetes mellitus. Outdated, but still widespread classification according to the necessary form of therapy.
- NIDDM: Abbreviation for non insulin dependent diabetes mellitus. Outdated, but still widespread classification according to the necessary form of therapy.
Questions and answers
Q: What is diabetes insipidus?
A: Diabetes insipidus is a disease that is unrelated to diabetes mellitus.
Q: What do people usually mean when they say "diabetes"?
A: When people say "diabetes", they usually mean diabetes mellitus.
Q: What are diabetics called?
A: People with diabetes Mellitus are called "diabetics".
Q: What is glucose?
A: Glucose is a natural carbohydrate that our bodies use as a source of energy. It is different from the kind of sugar sold in supermarkets, which is called sucrose. High concentrations of glucose can be found in soft drinks and fruits.
Q: How does the body control the glucose level in the blood?
A: The glucose level in the blood is controlled by several hormones. Hormones are chemicals in the body that send messages from cells to other cells. Insulin, which is made by the pancreas, sends a message to other cells in the body when you eat telling them to take up glucose from the blood for energy or store it as glycogen for later use.
Q: How does insulin work?
A: Insulin tells cells to take up glucose from the blood and use it for energy or store it as glycogen for later use when you eat. When you are not eating, cells break down stored glycogen into glucose to use as energy.
Q: Where can high concentrations of glucose be found?
A: High concentrations of glucose can be found in soft drinks and fruits.
Related articles
Author
AlegsaOnline.com Diabetes mellitus Leandro Alegsa
URL: https://en.alegsaonline.com/art/27072
Sources
- faqs.org : "What is glucose? What does "bG" mean?"