Designer baby: concepts, methods, and ethical questions
Overview of the concept of 'designer babies' including scientific methods (IVF, PGD, gene editing), potential applications, history, and ethical, legal, and social concerns.
The phrase "designer baby" is used in public and academic discussion to describe efforts to influence an unborn child's traits beyond routine medical care. It is a shorthand that covers a range of practices aimed at selecting, preventing, or altering inherited characteristics before or just after conception. The expression conveys cultural anxieties as much as scientific possibilities and is not a precise technical term.
Image gallery
6 Images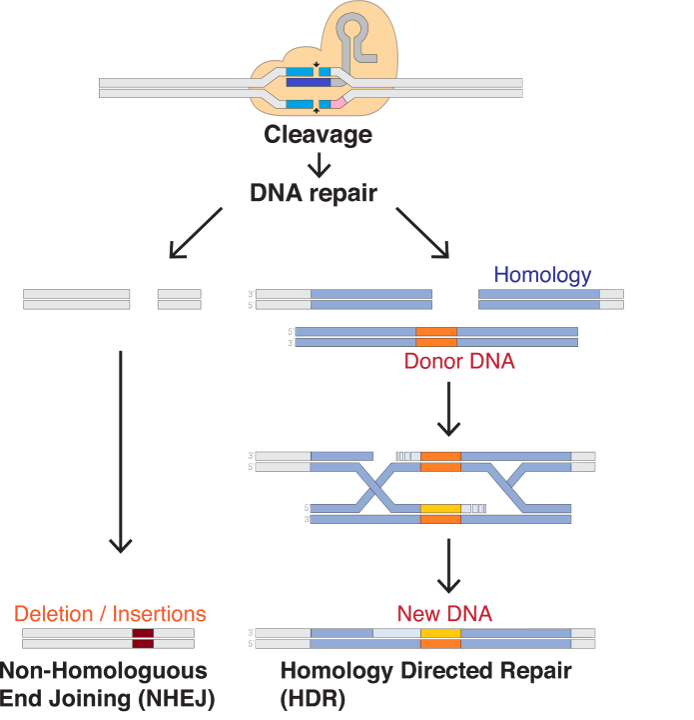





What the term covers
In practice, discussions of designer babies include two broad approaches: selection and genetic modification. Selection uses reproductive technologies to choose embryos or gametes with particular genetic profiles. Modification changes DNA or other biological material to alter traits that will be inherited by the child.
- Selection examples: in vitro fertilization (IVF) combined with preimplantation genetic diagnosis (PGD) to avoid severe hereditary disorders.
- Modification examples: gene editing tools (such as CRISPR) and mitochondrial replacement techniques that alter genetic material directly.
Scientific methods and limitations
Techniques relevant to the topic range from well-established clinical procedures to experimental laboratory methods. IVF and PGD are established and licensed in many countries for preventing single-gene diseases. Emerging tools like CRISPR enable targeted changes in DNA but remain technically challenging, especially when applied to human embryos or germline cells. Many changes have uncertain effects because genes interact in complex ways with environment and development. For accessible summaries, see genetic technologies.
Potential uses and examples
Medical aims are the most widely discussed: preventing life-threatening inherited conditions, reducing the risk of certain diseases, and avoiding mitochondrial disorders. Other proposed uses include modifying traits associated with metabolism, immune function, or physical characteristics. In practice, most clinical applications today focus on avoiding or reducing serious disease rather than enhancing complex traits such as intelligence or personality.
Ethical, legal and social considerations
The idea of designing human traits raises many questions. Critics point to risks of harm, unintended consequences, and widening social inequality if such services become available only to some. Concerns also include consent (the future person cannot consent to changes), the welfare of children, and impacts on diversity and disability communities. Legal regimes differ: some jurisdictions ban germline modification, others allow limited clinical research or regulate embryo selection practices. Public engagement and careful regulation are widely recommended by ethicists and scientists.
History and current status
Interest in controlling heredity has deep roots, but modern discussions accelerated with IVF and molecular genetics in the late 20th century and with programmable gene editing in the 21st century. Some interventions are already used clinically to prevent inherited disease; others remain experimental and are subject to research oversight and legal restriction in many countries.
Distinctions and notable facts
Important distinctions include the difference between somatic (non-heritable) therapies and germline (heritable) changes, and between selecting embryos and actively editing genomes. The term "designer baby" often blurs these differences, so precise language is essential when discussing science, policy, and ethics.
Questions and answers
Q: What is a designer baby?
A: The term designer baby refers to influencing the quality of an unborn child, usually by changing the genetics.
Q: What does influencing the quality of an unborn child mean?
A: It means changing the nature, usually the genetics, of the child for the better.
Q: Are there any issues associated with the idea of designer babies?
A: Yes, there are many technical, social, moral, and legal issues connected to the idea.
Q: Has society thought about the issues connected to the idea of designer babies?
A: No, society has scarcely begun to think about these issues.
Q: Can some of the ideas related to designer babies be done?
A: Yes, it is now certain that some of these ideas can, in principle, be done.
Q: What is the purpose of the brief survey mentioned in the text?
A: The purpose of the brief survey is to outline what might be done with regards to designer babies, but it is not a list of what should or will be done.
Q: Are some elements of designer babies already happening in some parts of the world?
A: Yes, some elements of designer babies are already happening in some parts of the world.
Related articles
Author
AlegsaOnline.com Designer baby: concepts, methods, and ethical questions Leandro Alegsa
URL: https://en.alegsaonline.com/art/26846
Sources
- online.wsj.com : "A baby please: blond, freckles -- hold the colic"
- telegraph.co.uk : "Designer babies: Controversy over embryo selection"
- washingtonpost.com : "Scientists see potential in amniotic stem cells"
- nature.com : "Isolation of amniotic stem cell lines with potential for therapy"
- doi.org : 10.1038/nbt1274
- pubmed.ncbi.nlm.nih.gov : 17206138
- biocellcenter.com : "Stem cells – BiocellCenter" · web.archive.org · web.archive.org
- doi.org : 10.1097/01.AOG.0000240135.13594.07
- pubmed.ncbi.nlm.nih.gov : 17077226
- reuters.com : "European biotech company Biocell Center opens first United States facility for preservation of amniotic stem cells in Medford, Massachusetts | Reuters" · web.archive.org
- boston.com : "Europe's Biocell Center opens Medford office – Daily Business Update – The Boston Globe"