Crohn's disease: overview, symptoms, causes, diagnosis and management
Crohn's disease is a chronic inflammatory condition of the digestive tract. This article summarizes its presentation, probable causes, diagnostic approach, treatment options, history and practical considerations.
Overview
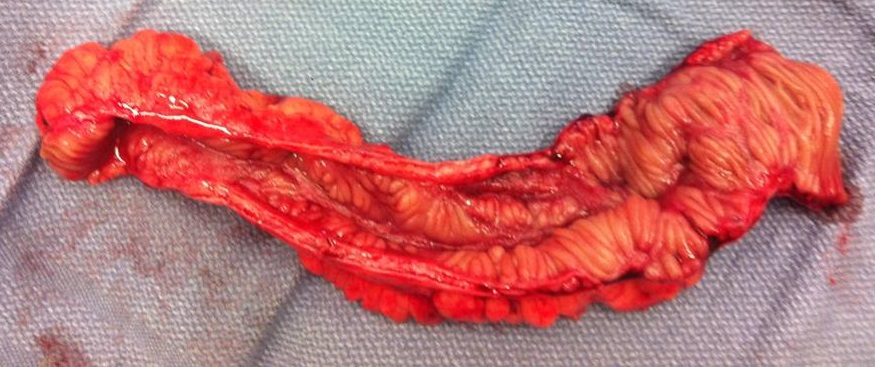
Crohn's disease is a long‑term inflammatory disorder that primarily affects the digestive tract. It belongs to the family of inflammatory bowel diseases (IBD) and most commonly involves portions of the small and large intestines. In affected areas the lining and deeper layers of the gut become inflamed and can develop small breaks or ulcers. The pattern of inflammation is often patchy, with healthy segments between inflamed segments, and disease severity varies widely between people.
Image gallery
10 Images






Symptoms and complications
Crohn's disease is a chronic condition that tends to follow a relapsing and remitting course: periods of active symptoms are followed by partial or complete remissions. Typical gastrointestinal complaints include abdominal pain, frequent loose stools or diarrhea, nausea or vomiting, and unintended weight loss. Beyond the gut, the disease can cause problems in other organs.
- Common extraintestinal manifestations: joint pain or arthritis, skin rashes, eye inflammation and mouth sores.
- Local complications: strictures (narrowing), fistulas (abnormal connections), abscesses and malabsorption of nutrients.
- Systemic effects: anemia, fatigue and growth delay in children.
Causes and risk factors
The exact origin of Crohn's disease is not fully understood. Most experts believe the illness results from an abnormal immune reaction: components of the immune system respond inappropriately to microbes in the gut. Although immune dysfunction is central, Crohn's is usually described as immune‑mediated rather than a classic autoimmune disease because the triggers involve environmental and microbial factors as well as host responses. Genetic predisposition plays a role: family history and certain inherited variants increase susceptibility (genetics).
Diagnosis and treatment
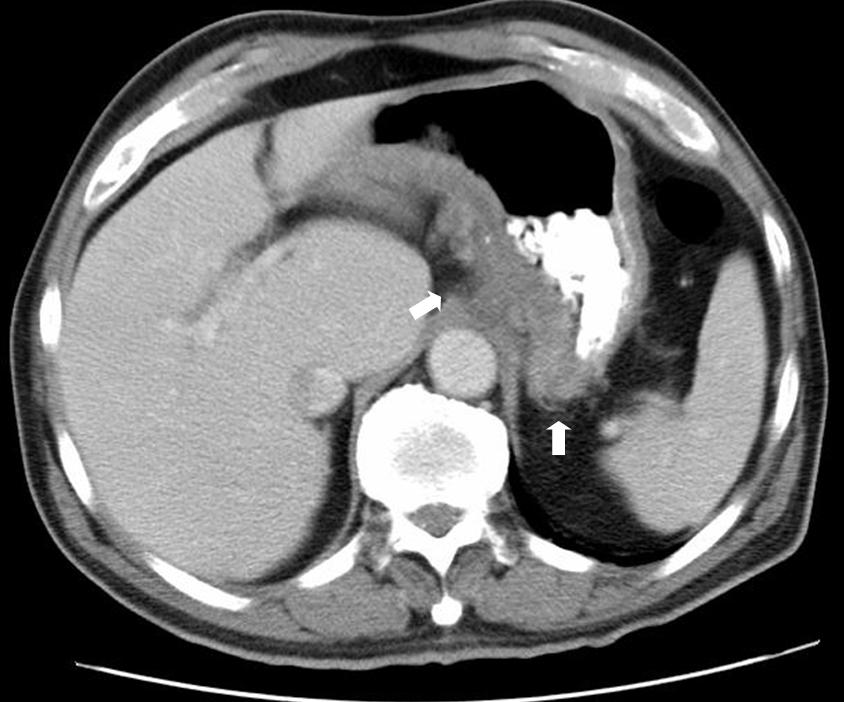
Diagnosis combines clinical history, physical examination and investigations such as blood tests, stool studies, endoscopy with biopsy, and cross‑sectional imaging. Management aims to control inflammation, relieve symptoms and prevent complications. Approaches include:
- Medications: anti‑inflammatory agents, immune modulators and biologic therapies are commonly used to reduce intestinal inflammation (medication).
- Nutrition and lifestyle: dietary adjustments, smoking cessation and other lifestyle measures can support treatment and reduce flares.
- Surgery: reserved for complications such as obstruction or uncontrolled fistulae; it treats problems but does not cure the underlying tendency to inflammation.
Some unconventional approaches and complementary therapies have been explored, including experimental use of helminths and a variety of alternative strategies; evidence for these options remains limited or mixed (alternative medicine).
History and ongoing research
The condition bears the name of Burrill B. Crohn, who, with colleagues, published a formal description in the early 1930s, although clinicians had noted similar intestinal disorders earlier in medical literature. Research continues to investigate how genes, the intestinal microbiome and environmental exposures interact to trigger and perpetuate the disease. Newer biologic agents, small molecules and precision‑medicine strategies aim to improve outcomes and reduce reliance on long‑term steroids and surgery.
Living with Crohn's disease
With current therapies many people achieve prolonged symptom control and maintain active lives, but individual courses vary. Regular follow up, timely treatment of flares and attention to nutrition, mental health and preventive care are important components of management. Reliable, up‑to‑date information and support are available from specialist clinics and patient organizations (learn more).
Questions and answers
Q: What is Crohn's disease?
A: Crohn's disease is a type of inflammatory bowel disease (IBD) that causes the intestines to become swollen and develop ulcers. It can cause pain in the stomach, diarrhea, vomiting, weight loss, skin rashes, arthritis and swollen eyes.
Q: Who first described cases of Crohn's disease?
A: Burrill Bernard Crohn first described cases of Crohn's in 1932. However Giovanni Battista Morgagni was the first to describe it in the 18th century.
Q: What causes Crohn's disease?
A: The exact cause of Crohn's disease is not known but it seems to be connected to a person's genes as people whose siblings have it are more likely to get it. It is also thought that an underlying immune problem may be involved where the body attacks itself causing swelling in the digestive tract.
Q: Is there a cure for Crohn's Disease?
A: Unfortunately there is no cure for Crohn's Disease at this time however managing it includes lifestyle changes and various kinds of medication.
Q: Are men or women more likely to get Crohn’s Disease?
A: Both men and women can be affected by Crohn’s Disease so neither gender has an increased risk over the other.
Q: Does alternative medicine help with treating symptoms ofCrohns Disease?
A: Alternative medicine such as certain parasitic intestinal worms appear to make the bowel less inflamed but its effects are uncertain so results vary from person to person.
Related articles
Author
AlegsaOnline.com Crohn's disease: overview, symptoms, causes, diagnosis and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/24272
Sources
- ncbi.nlm.nih.gov : PMID 21530736
- ncbi.nlm.nih.gov : PMID 19437144
- ncbi.nlm.nih.gov : PMID 20594136
- ncbi.nlm.nih.gov : PMID 18587394