Cornea: Structure, Function, and Clinical Importance
Transparent, avascular front tissue of the eye that provides most refractive power; layered microstructure, physiology, common diseases, and surgical treatments central to vision.
Overview
The cornea is the transparent, curved tissue that forms the front surface of the eye. It covers the iris and the pupil, provides a protective barrier, and allows light to enter the internal optical system. Because of its shape and refractive index, the cornea contributes the majority of the eye's focusing power and works together with the lens to form an image on the retina. The tissue is normally clear, avascular, and richly innervated.
Image gallery
7 Images
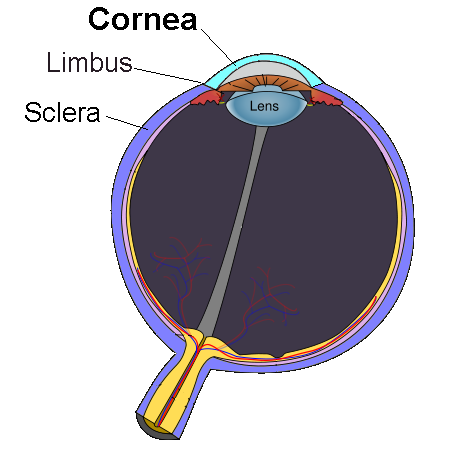




Structure and layers
The cornea is organized in multiple layers that together maintain transparency, strength and metabolic balance. From front (external) to back (internal) these are commonly described as:
- Epithelium — a thin, regenerative surface layer that protects against infection and maintains a smooth optical surface.
- Bowman’s layer — an acellular, tough zone beneath the epithelium that contributes mechanical stability.
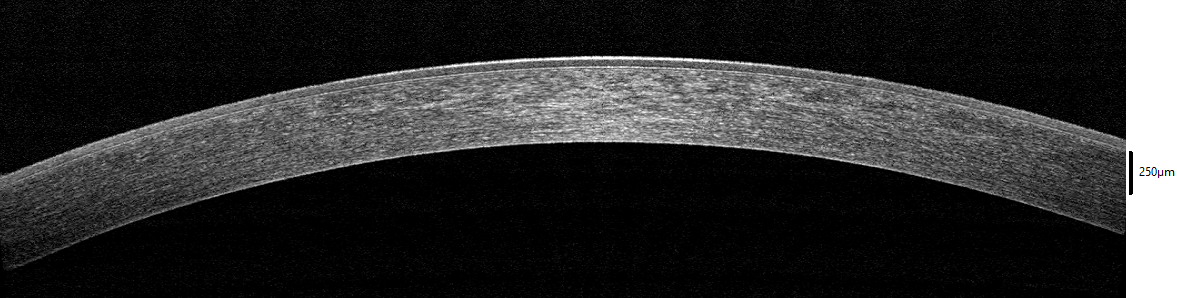
- Stroma — the thickest layer, composed of regularly arranged collagen lamellae and keratocytes; its ordered structure is essential for transparency.
- Dua’s layer — a thin lamina described in 2013 between deep stroma and Descemet’s membrane; its recognition prompted discussion among researchers and clinicians about whether it should be regarded as a separate anatomical layer and how it may influence surgical technique.
- Descemet’s membrane — a resilient basement membrane produced by the endothelium that supports posterior architecture.
- Endothelium — a single layer of metabolically active cells that pumps excess fluid from the stroma to maintain deturgescence and clarity.
Corneal nerves are unusually dense and lack external myelin sheaths, which preserves transparency while providing high sensitivity for reflexes such as blinking and tearing.
Optical and physiological roles
Optically, the cornea refracts incoming light (refraction) due to the change in curvature and refractive index at the air-tear interface; small changes in curvature or thickness can produce noticeable shifts in vision. Biologically, the cornea forms a barrier against pathogens and physical injury, contributes to a stable tear film, and supports ocular surface homeostasis. Because it is avascular, the cornea receives oxygen from the air via the tear film and nutrients from the aqueous humor and tears.
Common conditions and clinical testing
Disorders affecting the cornea range from acute injuries and infections (keratitis) to chronic degenerations and hereditary dystrophies. Examples include corneal abrasions, bacterial or viral ulcers, keratoconus (progressive thinning and cone-shaped deformation), and endothelial failure leading to corneal edema. Contact lens wear, dry eye, trauma, and autoimmune disease can all affect corneal health.
Clinicians assess corneal integrity and function using slit-lamp examination, corneal topography and tomography to map curvature, pachymetry to measure thickness, specular microscopy to evaluate endothelial cells, and staining techniques to reveal epithelial defects. These tests guide management and surgical planning.
Treatment and surgical options
Treatment depends on the condition. Infections require antimicrobial therapy; lubrication and anti-inflammatory measures address surface disease. For refractive errors, procedures that reshape the cornea (for example, laser-based techniques) alter its refractive power. For advanced or vision-threatening disease, surgical replacement of corneal tissue is common. Options include penetrating keratoplasty (full-thickness graft) and lamellar procedures that selectively replace diseased layers, such as posterior lamellar transplants that restore the endothelium while preserving healthy anterior tissue.
Recent developments and practical considerations
Descriptions of microanatomical features such as Dua’s layer stimulated examination of surgical methods and biomechanical behavior, though some debate about its status as a distinct layer continues. Modern corneal care emphasizes early diagnosis, preservation of the endothelium when possible, and use of tissue-sparing surgical approaches. Rehabilitation of vision after corneal disease may include optical correction, contact lenses, or transplantation, supported by postoperative management to prevent infection and rejection.
Further resources
- Introductory anatomical overviews of the eye and ocular surface.
- Technical discussions of corneal transparency and optics and how stromal structure determines clarity.
- Clinical guidance on the pupil, intraocular relationships and surgical planning.
- Information about nerve anatomy and myelin-related considerations at corneal innervation.
- Material on optical principles such as refraction and how corneal curvature affects focus.
- Practical clinical resources about retinal consequences of refractive error and posterior segment evaluation at retina and vision.
The cornea remains a central focus of ophthalmic research and care because its transparent, avascular nature is critical for vision and because small structural changes can have large functional effects. Early recognition and appropriate management of corneal disease preserve vision and improve quality of life.
Questions and answers
Q: What is the cornea?
A: The cornea is the front part of the eye that covers the iris, pupil, and eye chamber. It is a clear, transparent section of the eye.
Q: Does the cornea have blood vessels?
A: No, the cornea does not have blood vessels.
Q: What is the function of the cornea?
A: The cornea, along with the lens, refracts light and bends it so that the image strikes the retina. The cornea does about two-thirds of this refraction.
Q: What is Dua's layer?
A: Dua's layer is a newly discovered layer of the cornea, described in June 2013. It is the sixth layer of the cornea to be discovered.
Q: What is the strength of Dua's layer?
A: Despite its thinness, Dua's layer is very strong and air does not get through it.
Q: Does the cornea have nerves?
A: Yes, the cornea has nerves, but they do not have myelin sheaths on them.
Q: What is the role of the cornea and the lens in the eye?
A: The cornea and the lens work together to refract light and focus it onto the retina, allowing us to see objects clearly.
Related articles
Author
AlegsaOnline.com Cornea: Structure, Function, and Clinical Importance Leandro Alegsa
URL: https://en.alegsaonline.com/art/23129
Sources
- aaojournal.org : aaojournal.org/article/S0161-6420(13)00020-1/abstract
- medicaldaily.com : "New cornea layer discovered in human eye: doctors predict safer and simpler eye treatments"
- huffingtonpost.com : "New layer of human eye,'Dua's layer', discovered behind cornea"