Cardiac muscle (myocardium): structure, function, and clinical importance
Cardiac muscle (myocardium) is the involuntary, striated muscle of the heart. This article explains its structure, cellular features, physiology, blood supply, embryology, and how it differs from skeletal and smooth muscle.
Overview
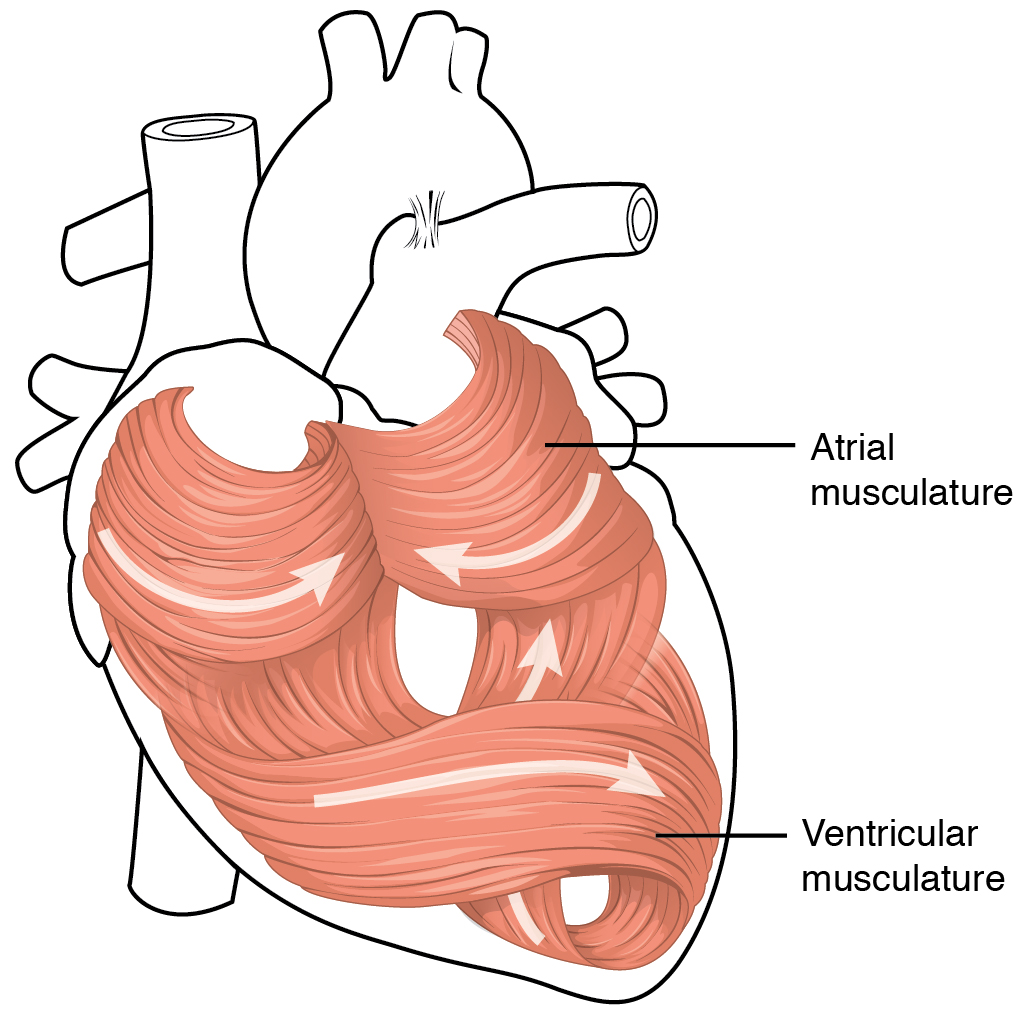
Cardiac muscle, commonly called heart muscle, forms the myocardium — the thick contractile layer of the heart wall. It is a specialized, striated muscle that operates involuntarily: people cannot control heart contractions consciously. The myocardium lies between the outer epicardium and the inner endocardium and is organized to pump blood effectively through the pulmonary and systemic circulations.
Image gallery
9 Images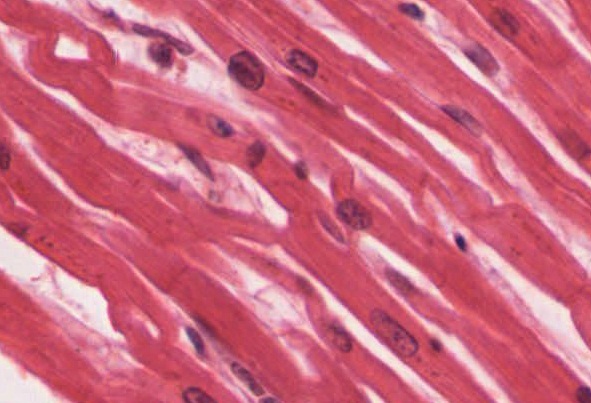







Structure and cellular characteristics
Cardiac muscle fibres are branched and connected end-to-end. Individual cardiac muscle cells (cardiomyocytes) typically contain a single nucleus, though some contain two. Cells are characterized by regular cross-striations like skeletal muscle, but they differ in shape and connectivity. Adjacent cardiomyocytes are joined by intercalated discs, complex junctions that include:
- desmosomes for mechanical strength, and
- gap junctions that permit electrical currents to pass directly between cells.
These features allow rapid, coordinated spread of electrical excitation and force across the myocardium. Cardiomyocytes also contain abundant mitochondria and an extensive sarcoplasmic reticulum to meet high and continuous energy and calcium-handling needs.
Function and physiological mechanisms
The principal role of cardiac muscle is to generate rhythmic contractions that move blood out of the atria and ventricles (systole) and then allow filling (diastole). Unlike skeletal muscle, cardiac tissue is intrinsically rhythmic: specialized pacemaker cells in the sinoatrial node and conduction pathways set the timing of contraction and coordinate impulse transmission across the heart. Action potentials in cardiomyocytes are prolonged compared with those in skeletal muscle, and contraction relies on calcium-induced calcium release from intracellular stores.
Blood supply and metabolic demands
Cardiac muscle has very high and continuous metabolic demands. It depends primarily on the coronary arteries for delivery of oxygen and nutrients and for removal of metabolic waste. Because the heart cannot pause for long without pumping blood, myocardial tissue must receive an uninterrupted blood supply; interruption of coronary flow quickly compromises function and can cause irreversible injury.
Development, clinical relevance, and distinctions
Embryologically, the myocardium arises from mesodermal heart-forming fields and remodels into chambers and conduction tissue during development. Clinically, diseases of cardiac muscle include ischemic injury (myocardial infarction), inflammatory conditions, cardiomyopathies, and arrhythmias — problems that affect the heart’s ability to contract or to maintain a normal rhythm.
Compared with the other two major vertebrate muscle types, cardiac muscle shares striations with skeletal muscle but is involuntary like smooth muscle. Key distinctions include branching fibers and intercalated discs (cardiac), long multinucleated fibers under voluntary control (skeletal), and non-striated spindle-shaped cells organized for slower, sustained contractions (smooth).
Further reading and resources
- Role and regulation of involuntary contraction: involuntary control
- Striated appearance and microscopic features: striated muscle histology
- Comparison with other muscle types: skeletal muscle and smooth muscle
- Cellular composition and nuclei: cardiomyocyte nuclei
- Position of the myocardium in the heart wall: heart wall layers
- Coordinated contractions and electrical conduction: cardiac conduction
- How contractions move blood through circulatory systems: blood ejection
- Left and right heart roles in systemic and pulmonary circulation: systemic vs pulmonary
- Importance of coronary perfusion and limited diffusion: coronary circulation
Questions and answers
Q: What is a cardiac muscle?
A: A cardiac muscle is one of the three main types of muscle in vertebrates found in the walls of the heart.
Q: Is a cardiac muscle under voluntary control?
A: No, a cardiac muscle is involuntary, which means a person cannot control it consciously.
Q: What are the other two types of muscles, besides a cardiac muscle?
A: The other two types of muscles are the skeletal muscles and smooth muscles.
Q: What is the myocardium?
A: The myocardium is the tissue that makes up the thick middle layer of the heart.
Q: How does the coordinated contractions of cardiac muscles in the heart force blood out of the atria and ventricles?
A: The coordinated contractions of cardiac muscles in the heart force blood out of the atria and ventricles to the blood vessels of the left/body/systemic and right/lungs/pulmonary circulatory systems.
Q: What is systole?
A: Systole is the contraction of the heart which forces blood out of the atria and ventricles to the blood vessels of the left/body/systemic and right/lungs/pulmonary circulatory systems.
Q: How do cardiac muscle cells receive oxygen and nutrients and remove waste products?
A: Unlike most other tissues in the body, cardiac muscle cells rely on the coronary arteries to deliver oxygen and nutrients and remove waste products directly because there is no time for them to diffuse.
Related articles
Author
AlegsaOnline.com Cardiac muscle (myocardium): structure, function, and clinical importance Leandro Alegsa
URL: https://en.alegsaonline.com/art/16930
Sources
- sciencedirect.com : "Aging, cardiac hypertrophy and ischemic cardiomyopathy do not affect the proportion of mononucleated and multinucleated myocytes in the human heart"
- doi.org : 10.1006/jmcc.1996.0137
- pubmed.ncbi.nlm.nih.gov : 8841934
- mayoclinic.org : Left Ventricular Hypertrophy
- emedicine.medscape.com : Sinus Node Dysfunction
- mayoclinic.org : Coronary Artery Disease