West Nile virus (WNV): overview, transmission, history, and prevention
Comprehensive overview of West Nile virus (WNV), a mosquito-borne flavivirus that primarily infects birds but can cause human and animal disease; covers biology, transmission, symptoms, history, and prevention.
Overview
West Nile virus (WNV) is an RNA virus in the family Flaviviridae, genus Flavivirus. It causes a range of illness collectively known as West Nile virus disease. WNV naturally cycles between birds and mosquitoes and can incidentally infect mammals, including humans and horses. Most human infections are mild or asymptomatic, but the virus can occasionally produce serious neurologic disease.
Image gallery
10 Images







Characteristics and transmission
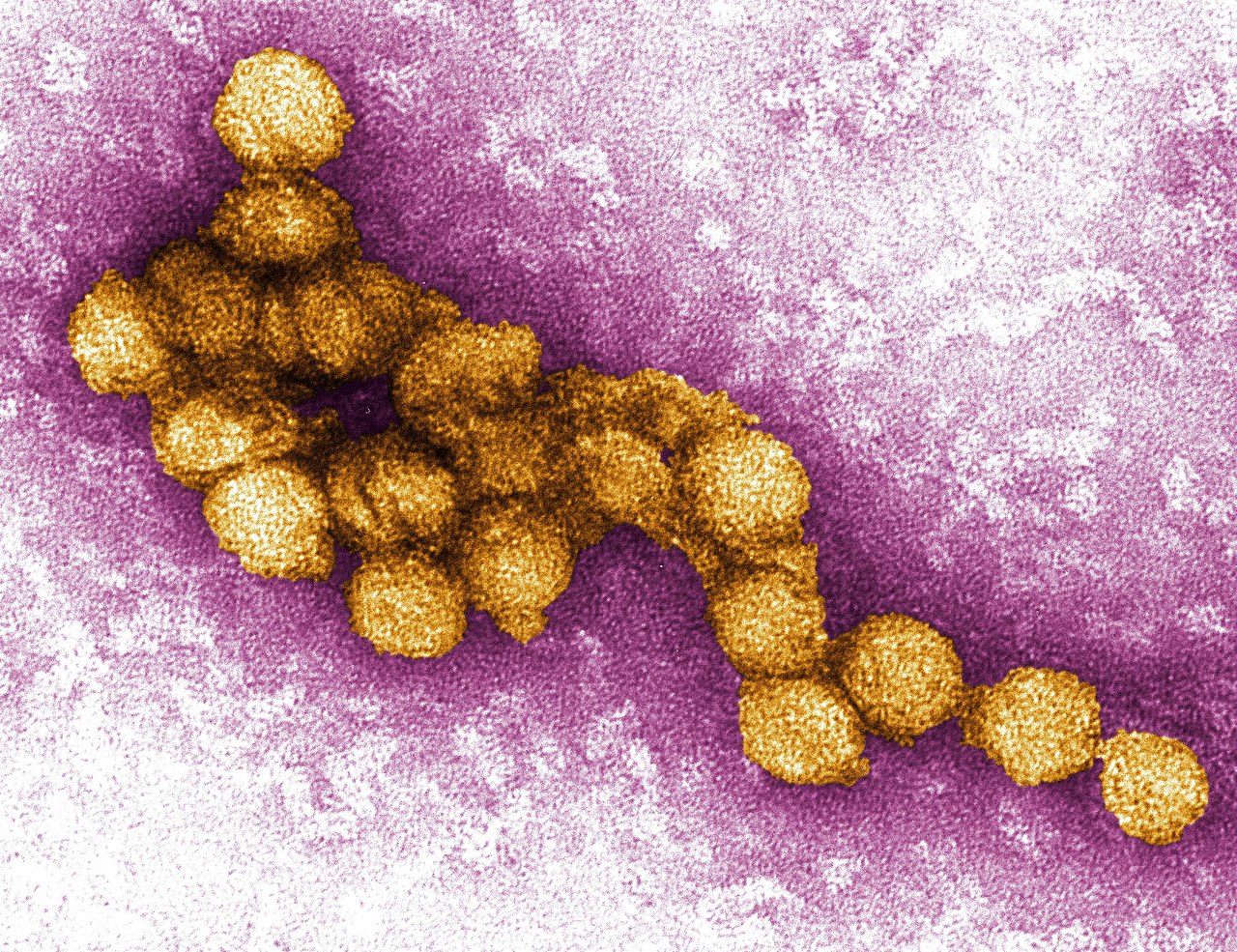
WNV is an enveloped, single-stranded positive-sense RNA virus. The natural transmission cycle involves ornithophilic mosquitoes that acquire the virus when feeding on infected birds; infected mosquitoes then spread the virus to additional birds and to incidental hosts. Humans and many mammals are generally dead-end hosts because they develop only low levels of virus in the blood and do not contribute significantly to onward transmission. Transmission routes are primarily mosquito bites, though rare cases have been associated with blood transfusion, organ transplantation, or vertical transmission.
Clinical features and diagnosis
Most infections are subclinical. Symptomatic illness ranges from a self-limited febrile syndrome with fever, headache, and muscle aches to severe neuroinvasive disease such as meningitis, encephalitis, or acute flaccid paralysis. Older adults and people with certain medical conditions are at greater risk for severe outcomes. Diagnosis is commonly by detection of specific antibodies or viral RNA in serum or cerebrospinal fluid; laboratory testing should be interpreted with clinical and epidemiologic context.
Prevention, control, and treatment
There is no specific antiviral therapy that is routinely recommended for WNV; care is mainly supportive. Prevention focuses on reducing mosquito exposure and population control: eliminating standing water where mosquitoes breed, using personal protective measures such as repellents and clothing barriers, and community vector control programs. Vaccines are available for horses but not for general human use, so public health measures and surveillance remain central to limiting spread.
History and geographic spread
WNV was first isolated in 1937 in the West Nile district of Uganda. For decades it was reported intermittently in Africa, parts of Europe, the Middle East, and Asia. Since the 1990s, more frequent outbreaks and wider distribution have been documented. The virus was detected in the Americas at the end of the 20th century and has since established local transmission in multiple regions. Large human outbreaks have occurred at various times and places, highlighting the virus's capacity for rapid geographic expansion.
Public health significance and notable distinctions
West Nile virus is important for veterinary as well as human health; bird mortality can be a sentinel for local transmission and horses may become seriously ill without vaccination. WNV belongs to the same genus as other medically significant viruses (for example, dengue and Zika), but differs in its primary bird–mosquito cycle and clinical patterns. Surveillance, rapid laboratory diagnosis, and integrated vector management are key elements in reducing human and animal disease burden.
Further information and resources
- General information about WNV
- Taxonomy: Flavivirus genus
- Flavivirus family details
- WNV and horses
- WNV and domestic animals
- WNV in bats
- WNV and cats
- WNV in reptiles
- WNV in amphibians
- Mosquito vectors and ecology
- Origins: Uganda
- East Africa context
- Historic outbreaks overview
- Outbreak information: Algeria
- Outbreak information: Romania
- Introduction to North America
- Caribbean reports
- Latin America surveillance
- Ongoing activity in Africa
- WNV in Asia
- Activity in Australia
- WNV in Europe
- Reports from the Middle East
- Canada: surveillance and cases
- United States: public health response
- Notable epidemics and impact
Note: This article summarizes broadly accepted information about West Nile virus. For clinical guidance, diagnosis, or local public health recommendations consult qualified health authorities.
Questions and answers
Q: What is West Nile Virus?
A: West Nile Virus (WNV) is a virus that belongs to the genus Flavivirus and causes an infectious disease called "West Nile virus disease" or just "West Nile virus."
Q: How does WNV spread?
A: WNV is mainly spread by mosquitoes, who get the virus from birds. If a mosquito bites a bird that has WNV, and then bites a human, that person can get West Nile Virus.
Q: Where was WNV first discovered?
A: West Nile virus was first discovered in 1937 in the West Nile area of Uganda, in East Africa.
Q: When did cases of WNV start to increase?
A: Before the 1990s there were very few cases of WNV, but then there was an outbreak in Algeria in 1994 and another in Romania in 1996. By 2004, the virus had spread to North America, the Caribbean islands, and Latin America.
Q: Where has WNV spread to since its discovery?
A: Since its discovery, WNV has continued to spread through Africa, Asia, Australia, Europe, the Middle East, Canada and the United States.
Q: What type of animals can be infected with WNV?
A: In addition to humans and birds being able to contract it from mosquitoes carrying it from other birds; horses , dogs , bats , cats , reptiles , and amphibians can also be infected with West Nile Virus .
Q: What year saw one of the worst epidemics yet for West Nile Virus ?
A: 2012 saw one of the worst epidemics yet for West Nile Virus ; 286 people died .
Related articles
Author
AlegsaOnline.com West Nile virus (WNV): overview, transmission, history, and prevention Leandro Alegsa
URL: https://en.alegsaonline.com/art/107421
Sources
- who.int : "West Nile virus"
- ncbi.nlm.nih.gov : "West Nile Virus Infection in Crocodiles"
- doi.org : 10.3201/eid0907.020816
- pubmed.ncbi.nlm.nih.gov : 12899140
- ncbi.nlm.nih.gov : "Alligators as West Nile Virus Amplifiers"
- doi.org : 10.3201/eid1012.040264
- pubmed.ncbi.nlm.nih.gov : 15663852
- mdpi.com : "Climate Change and West Nile Virus in a Highly Endemic Region of North America"
- doi.org : 10.3390/ijerph10073052
- ncbi.nlm.nih.gov : 3734476
- pubmed.ncbi.nlm.nih.gov : 23880729
- dx.doi.org : "West Nile virus, Texas, USA, 2012"
- doi.org : 10.3201/eid1911.130768