Ventricular tachycardia (VT): overview, causes, and management
Ventricular tachycardia (VT) is a rapid heart rhythm arising in the ventricles. This article explains its mechanisms, clinical features, diagnosis, emergency risks, and common treatments.
Overview
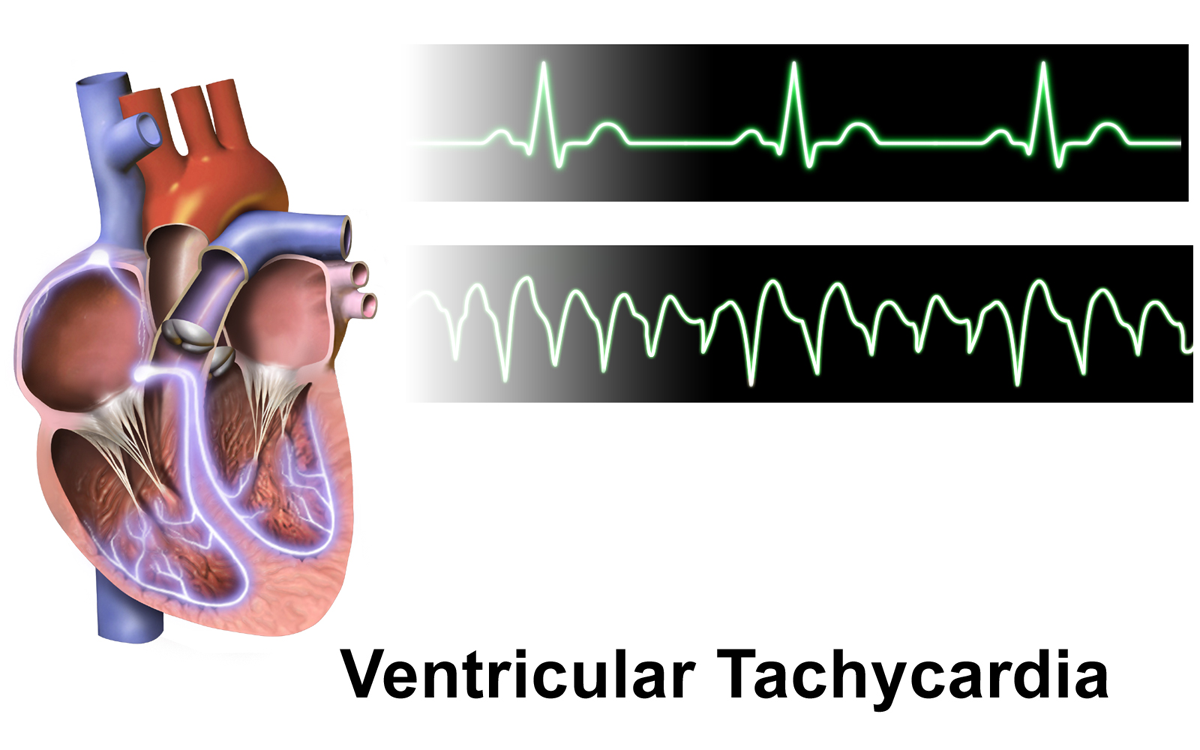
Ventricular tachycardia (VT or V‑tach) is a fast, abnormal heart rhythm that begins in the ventricles, the lower chambers of the heart. It is a form of tachycardia and represents a disruption of the heart's normal electrical sequence, in which the ventricles contract before or independently of the atria. Because the ventricles are the main pump for blood to the body, VT can quickly impair circulation and is often treated as a medical emergency.
Image gallery
4 Images


Mechanism and characteristics
Normally, electrical impulses originate in the atria and travel to the ventricles through a coordinated conduction system (heart anatomy). In VT, an abnormal focus, re‑entry circuit, or triggered activity within the ventricular muscle produces a rapid ventricular rate. The heart rate in VT is usually well above a normal resting range of 60–100 beats per minute, often fast enough that the ventricles do not have adequate time to fill with blood between beats. On an electrocardiogram, VT typically shows wide QRS complexes and a regular rapid rhythm; clinicians distinguish monomorphic VT from polymorphic VT and non‑sustained from sustained forms.
Causes and risk factors
- Structural heart disease — prior heart attack, scar tissue, or cardiomyopathy.
- Ischemia — reduced coronary blood flow that can provoke ventricular arrhythmias.
- Electrolyte disturbances (for example, abnormal potassium or magnesium).
- Drug effects or toxicity (some medications and stimulants).
- Inherited channelopathies and certain genetic syndromes.
These conditions change the electrical properties of the ventricular muscle and increase the chance of rapid, disorganized beating that can reduce cardiac output and cause hypotension (low blood pressure).
Clinical presentation and complications
Symptoms depend on the rate, duration, and underlying heart function. VT may cause palpitations, lightheadedness, chest pain, shortness of breath, or collapse. When the ventricles beat too rapidly, vital organs such as the brain receive less blood and oxygen, which can lead to fainting or altered mental status. VT can degenerate into ventricular fibrillation, progress to cardiac arrest, or result in sudden death if not rapidly treated.
Diagnosis and initial management
Diagnosis relies on clinical assessment and an electrocardiogram. In emergencies, securing the airway, breathing, and circulation is paramount. Immediate treatment depends on the patient's stability: unstable patients with severe symptoms or hypotension usually require prompt synchronized cardioversion or defibrillation. Stable patients may be managed with antiarrhythmic medications and monitoring while reversible causes (electrolyte imbalances, ischemia, drug effects) are corrected.
Long‑term treatment and prevention
- Implantable cardioverter‑defibrillators (ICDs) for patients at high risk of recurrent VT or sudden cardiac death.
- Catheter ablation targeting the arrhythmia focus for recurrent or drug‑refractory VT.
- Medications such as beta blockers or antiarrhythmics to reduce episodes.
- Management of underlying heart disease, lifestyle modification, and correction of metabolic causes.
Prognosis varies with the cause, the frequency of episodes, and how quickly treatment is provided. Early recognition, appropriate emergency response, and targeted long‑term strategies can markedly improve outcomes for people with ventricular tachycardia. For further information on related topics, see resources on tachycardia basics, heart structure (anatomy), emergency care (acute management), and complications such as ventricular fibrillation and sudden cardiac death.
Additional practical references include guidance on monitoring heart rate (normal and abnormal rates), maintaining circulatory volume (blood flow), recognizing hypotension (blood pressure), protecting organ perfusion (brain and oxygen delivery), and avoiding triggers that may precipitate ventricular arrhythmias.
Questions and answers
Q: What is ventricular tachycardia?
A: Ventricular tachycardia is a fast heart rate that occurs when the ventricles start to squeeze first due to the malfunctioning of electrical signals that tell the atria to squeeze first.
Q: What are the four chambers of the heart called?
A: The heart has four chambers that are called as atria and ventricles.
Q: What happens to the heart during ventricular tachycardia?
A: During ventricular tachycardia, the heart does not have enough time to refill with blood between beats as the electrical signals that tell the atria to squeeze first are not working.
Q: Why is ventricular tachycardia considered a medical emergency?
A: Ventricular tachycardia is considered a medical emergency because it can lead to low blood pressure, insufficient blood and oxygen supply to important body parts and can even cause sudden death.
Q: What is the normal heart rate?
A: The normal heart rate ranges from 60-100 beats per minute.
Q: At what rate do most people have heart rate in ventricular tachycardia?
A: Most people have a heart rate of at least 170 beats per minute in ventricular tachycardia.
Q: What are the potential risks associated with ventricular tachycardia?
A: Ventricular tachycardia can lead to low blood pressure, insufficient blood and oxygen supply to important body parts, ventricular fibrillation, and sudden death.
Related articles
Author
AlegsaOnline.com Ventricular tachycardia (VT): overview, causes, and management Leandro Alegsa
URL: https://en.alegsaonline.com/art/104590
Sources
- my.clevelandclinic.org : "Ventricular Tachycardia"
- doi.org : 10.1016/S0140-6736(12)61413-5
- pubmed.ncbi.nlm.nih.gov : 23101719
- doi.org : 10.1161/CIRCULATIONAHA.110.970954
- pubmed.ncbi.nlm.nih.gov : 20956222
- emedicine.medscape.com : "Ventricular Tachycardia"